12 Oct Hospital Rapid Response Teams: Why run when you can fly?
Hospital Rapid Response Teams: Why run when you can fly?
Today, Rapid Response Teams (RRTs) are a crucial component of many hospitals. Implementing a RRT was one of the six strategies that defined the Institute for Healthcare Improvement (IHI) 100,000 Lives campaign. Most RRTs consist of critical care nurses, but they can also include respiratory therapists, pharmacists, and physicians.
Research consistently shows that patients exhibit signs and symptoms of deterioration for several hours prior to a code. These symptoms include changes in vital signs, mental status, and lab markers. The goal of a RRT is to intervene upstream from a potential code. They reach the patient before deterioration turns into crisis. This is different than a code blue team that typically responds to a patient that has already decompensated to cardiac arrest.
Historically, most hospitals relied on busy bedside nurses to identify crashing patients and call for rapid response. With most states having no limits on the number of patients assigned per nurse, many medical-surgical ward nurses are caring for 6 or more patients per shift. Placing this additional responsibility on their already over-flowing plate is challenging at best. Providing a RRT empowers bedside nurses to trigger an escalation of care earlier and faster.
Measurable Improvement in Patient Outcomes
Hospitals using RRTs typically observe reductions in the number of cardiac arrests, unplanned transfers to the ICU, and overall mortality rate. A recent study of 471,062 patients showed a significant decrease in hospital mortality after implementation of a RRT. Other studies have shown reduction in hospital stay, ICU admissions, and non-ICU cardiorespiratory arrest.
UPMC McKeesport reports a decrease of code blues from 8 per month to 6 and an increase in survival rate of 40-60%. Half of the approximate 25 non-code calls received by their RRT each month result in early intervention and escalation of care – preventing further deterioration requiring a code.
Beyond Clinical Outcomes
There are also broader organizational benefits with implementing RRTs. Having the support and availability of an early intervention team significantly improves nurse satisfaction, and it provides a competitive advantage in recruiting and retaining nurses.
“In the old days, a nurse could struggle for 90 minutes with a failing patient,” says Michael White, MD, FACP, Senior Vice President for Value and Education at UPMC McKeesport. Despite following all the correct protocols, trying to reach the physician and waiting for diagnostic tests, isolated floor nurses are not actually escalating care for decompensating patients. The stress and frustration is significant for these nurses, and it also has an impact on their ability to care for their other patients.
Your Rapid Response Team Wants Wings
There is no question of improvement in patient care quality and outcomes with the implementation of RRTs, but many hospital leaders still want to see better metrics. Dana Edelson, the medical director of rescue care and resiliency at the University of Chicago believes there are two ways in which RRTs can be more successful: (1) Calling RRTs earlier and more often (2) Ensuring that when they get there they always do the right thing.
As in any industry, the way to guarantee that the same process is followed 100% of the time is to leverage technology to execute it. To that end, more and more hospitals are experimenting with augmenting their RRT programs with real-time, technology to automate rapid response triggers and minimize the risk of human error.
“An intelligent system that incorporates vital signs and triggers teams automatically could potentially lead to earlier detection than the current system of waiting for a clinician to get to the room, look at the patient, and decide if they need help,” says White.
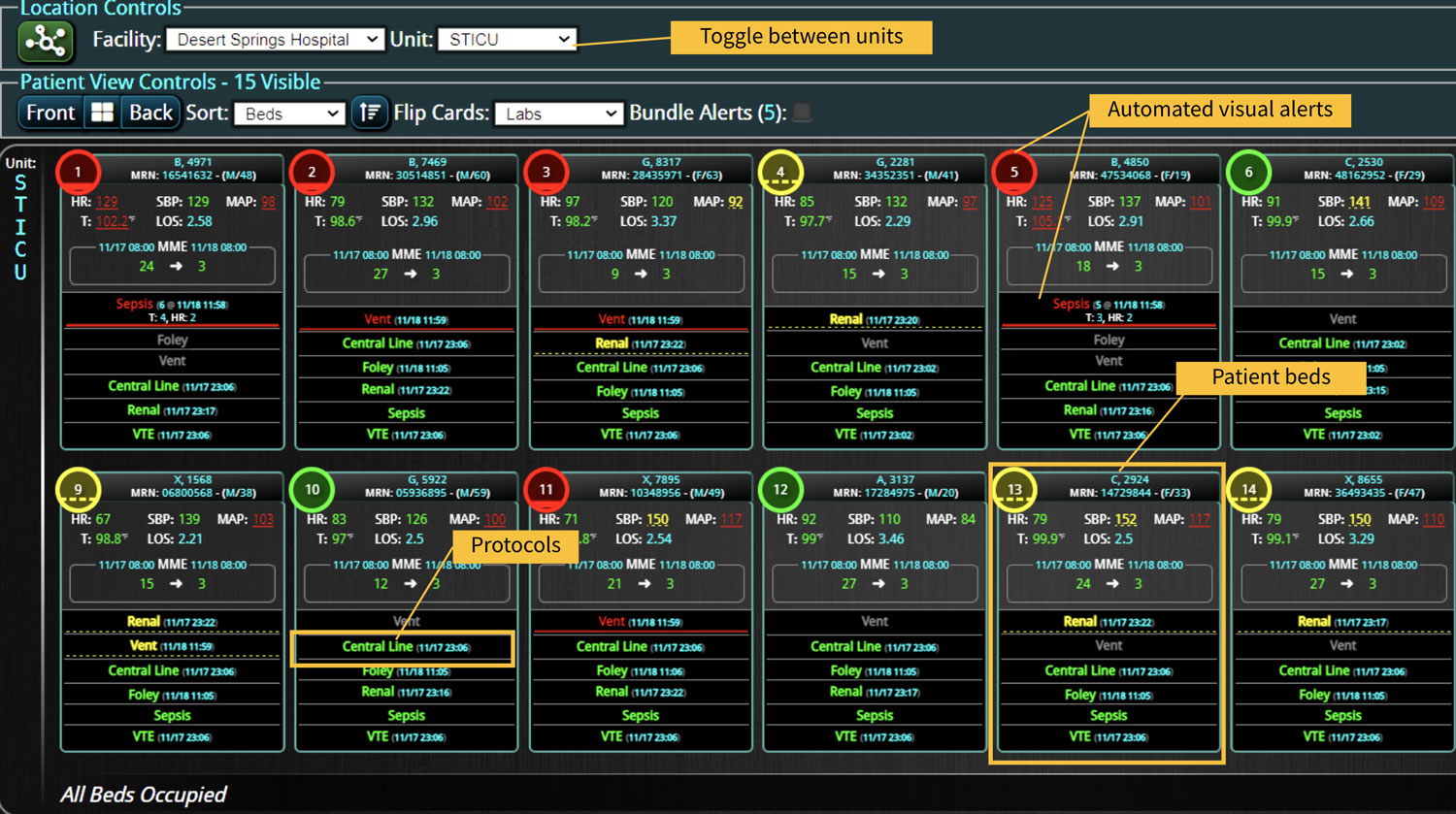
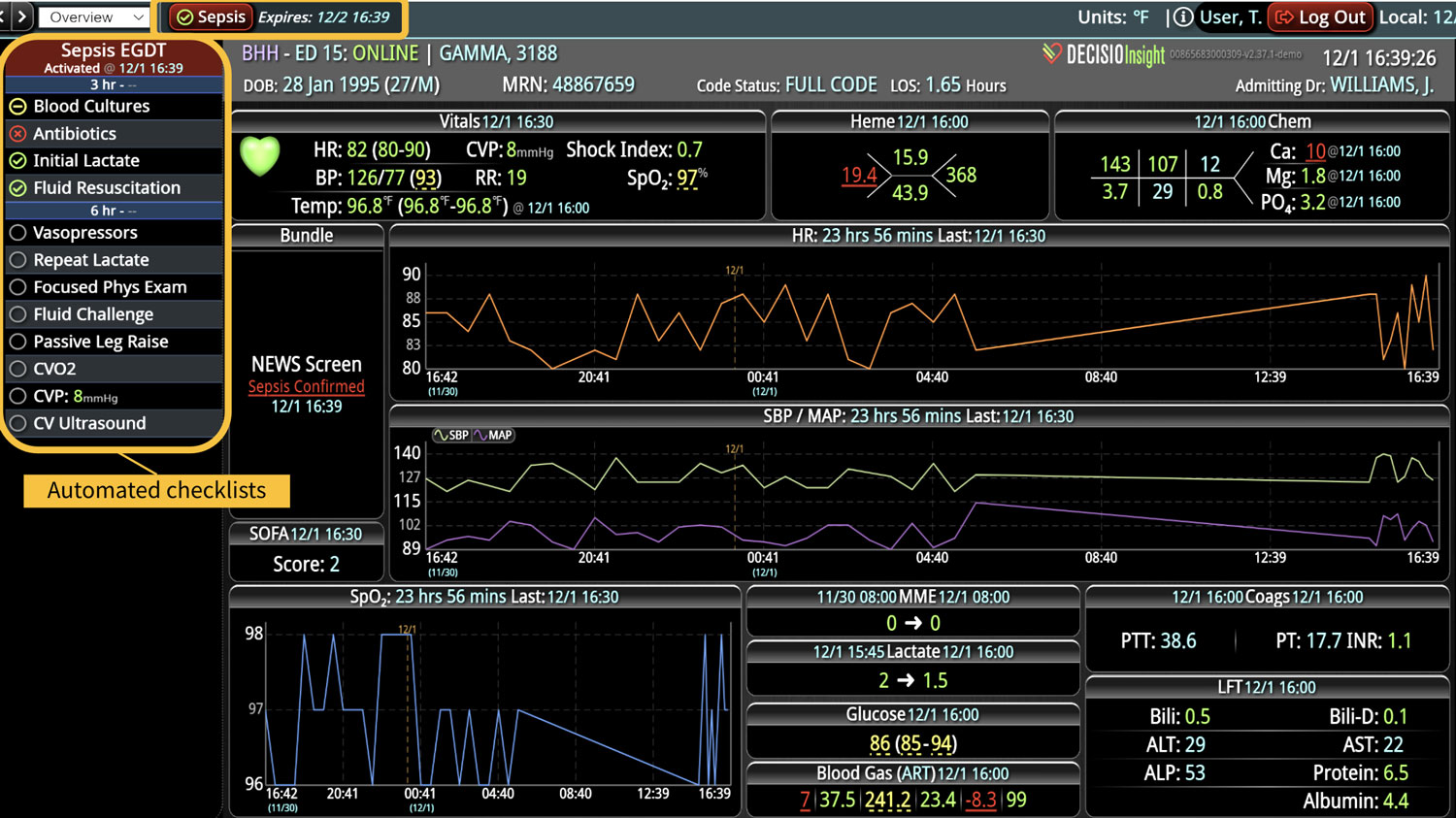
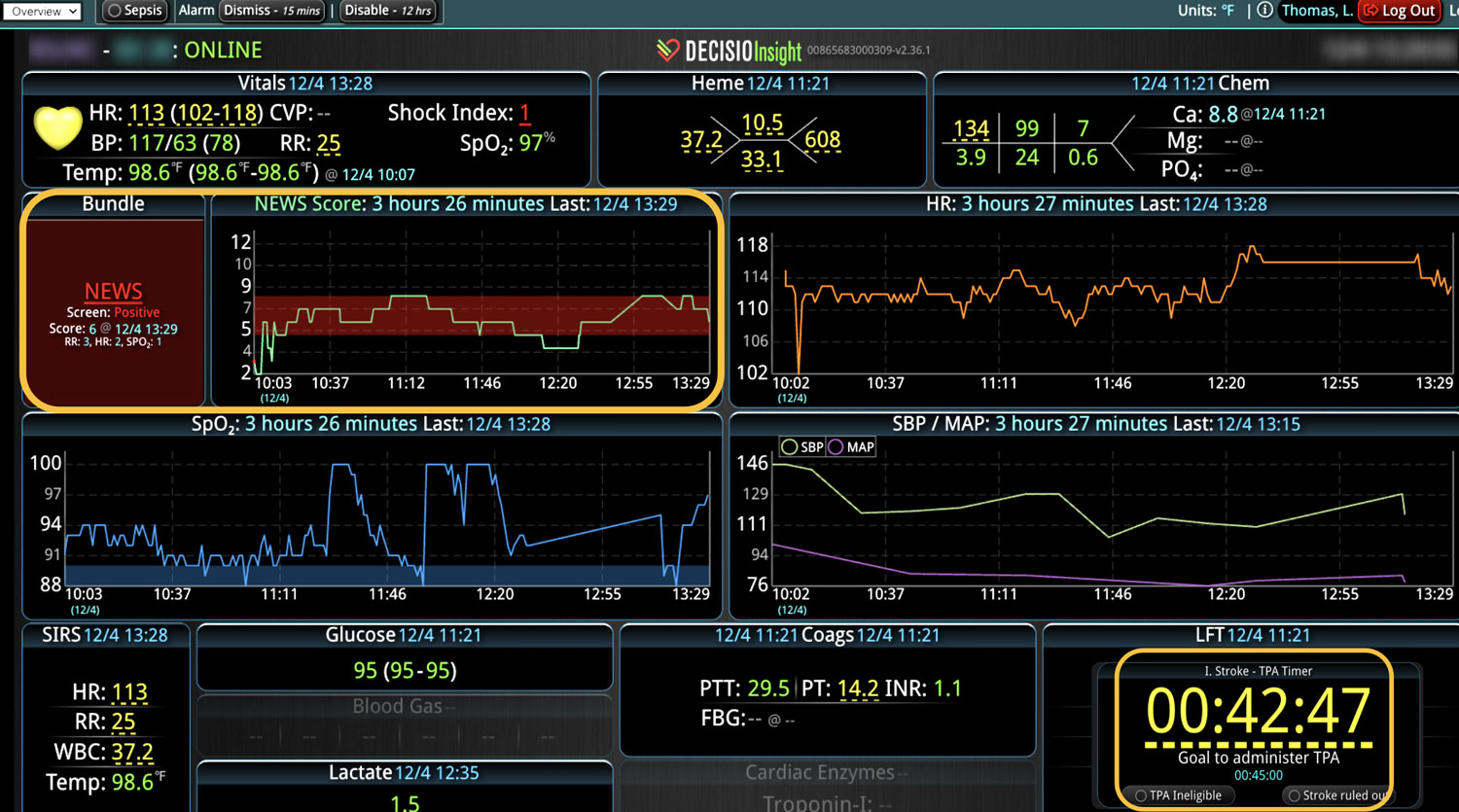
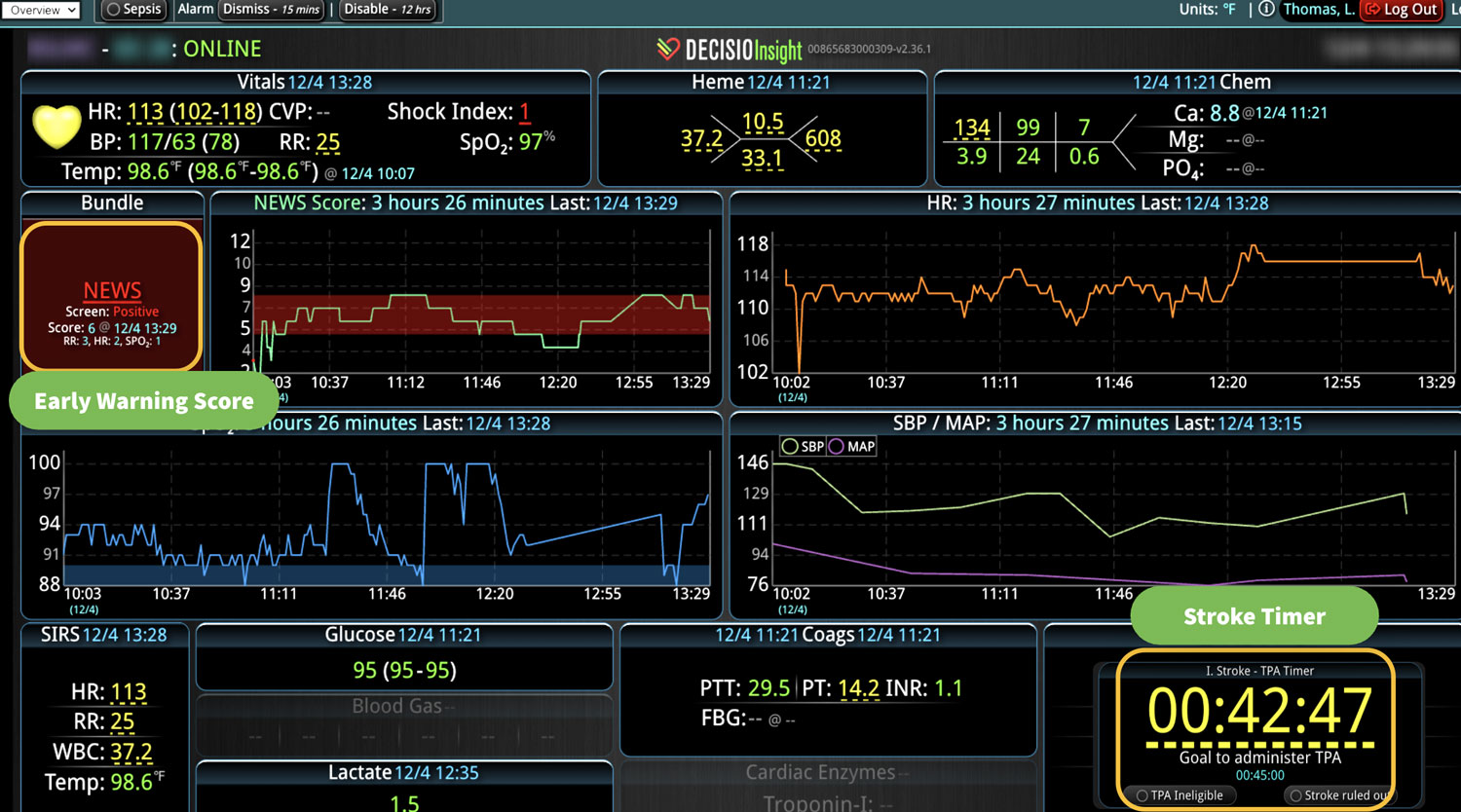
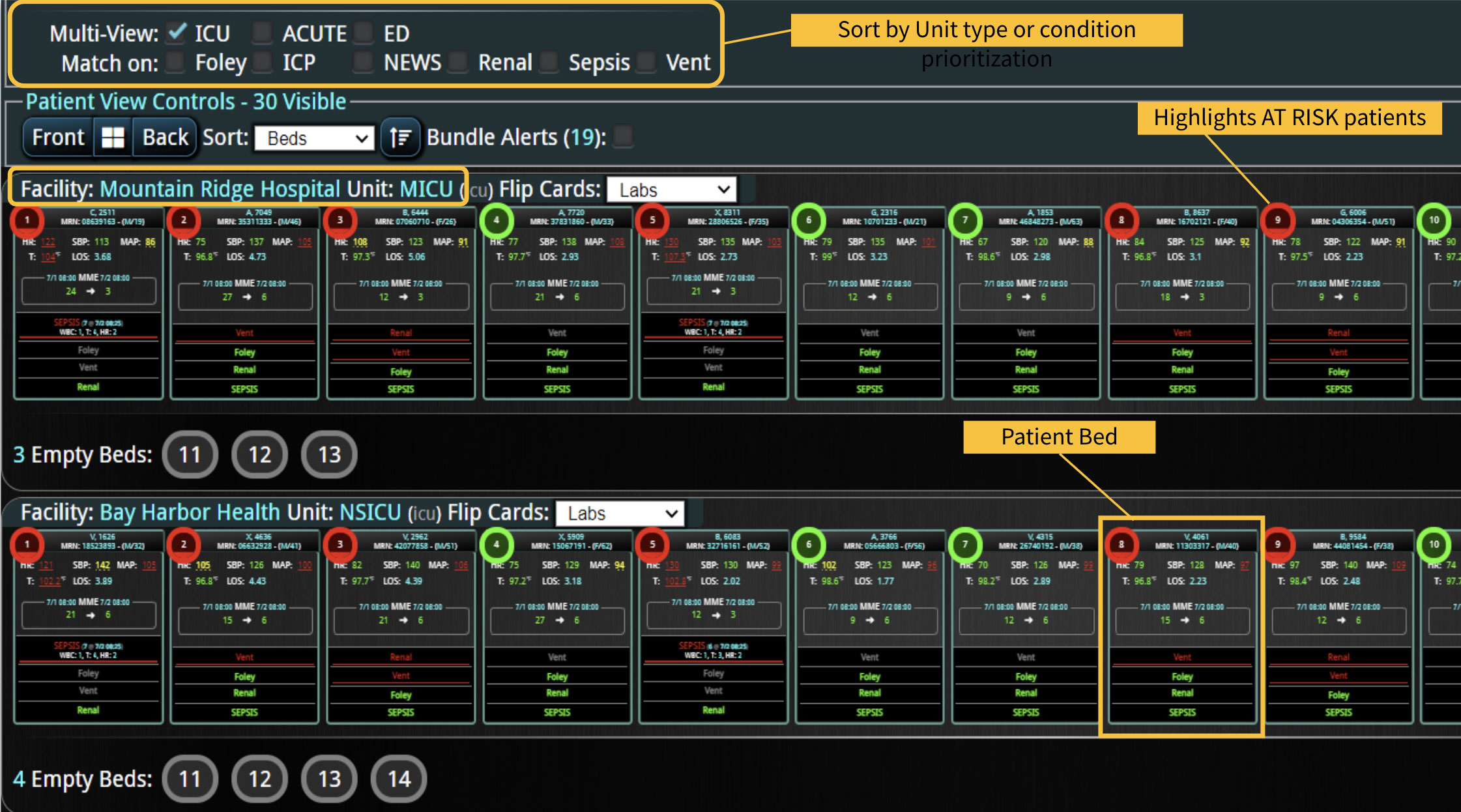
As hospitals investigate their options for rapid response technology, they are realizing that the EMR falls short of providing the meaningful, real-time, actionable triggers they’re looking for. In addition to the constant alert fatigue it generates, the EMR uses only a fraction of patient data floating within the hospital walls. Device, vitals, medications, and lab systems data are not factored into EMR logic. Additionally, the EMR does not truly automate this workflow because the trigger for the trigger is still manual! Someone must log in, open the record, and assess the alert before action is taken.
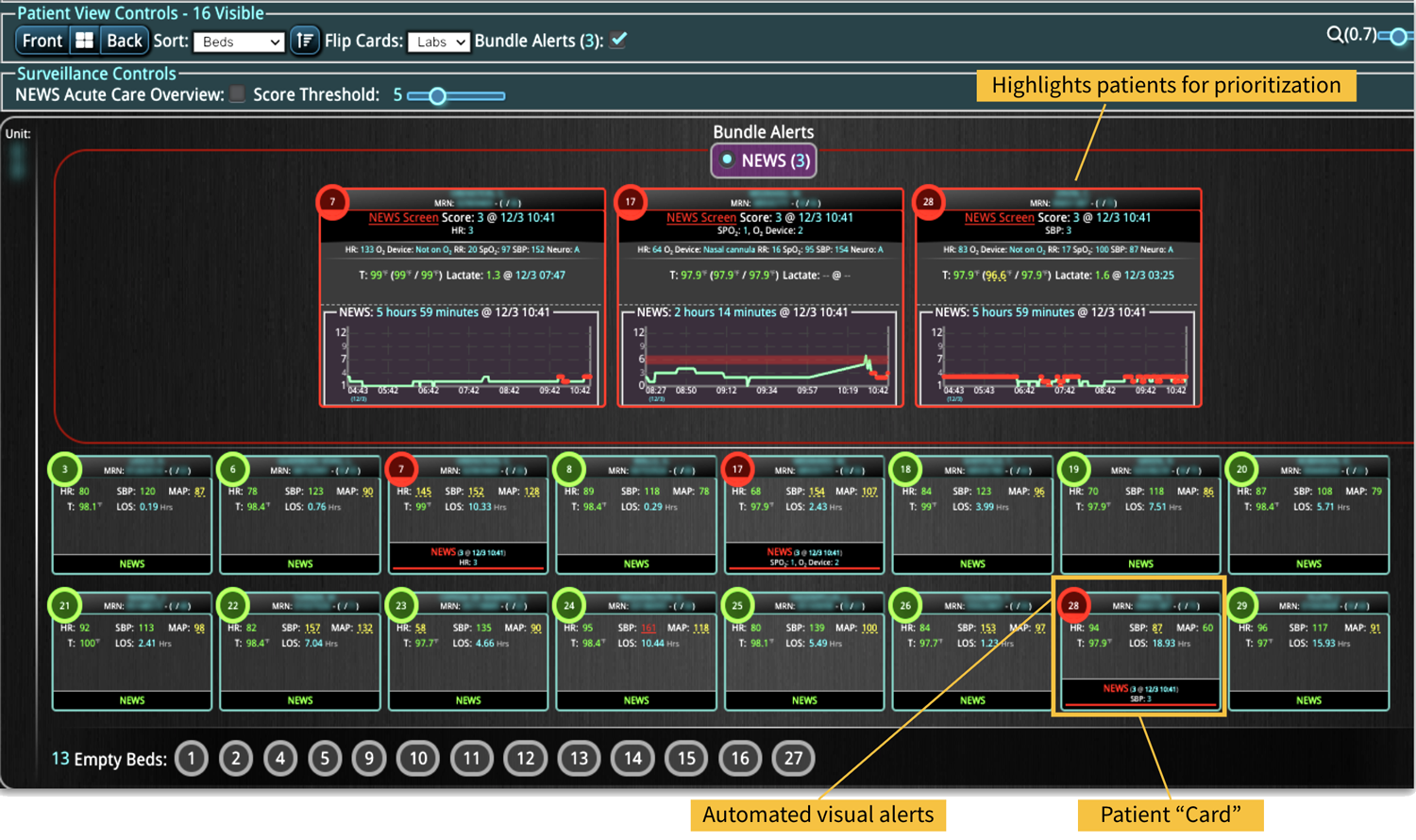
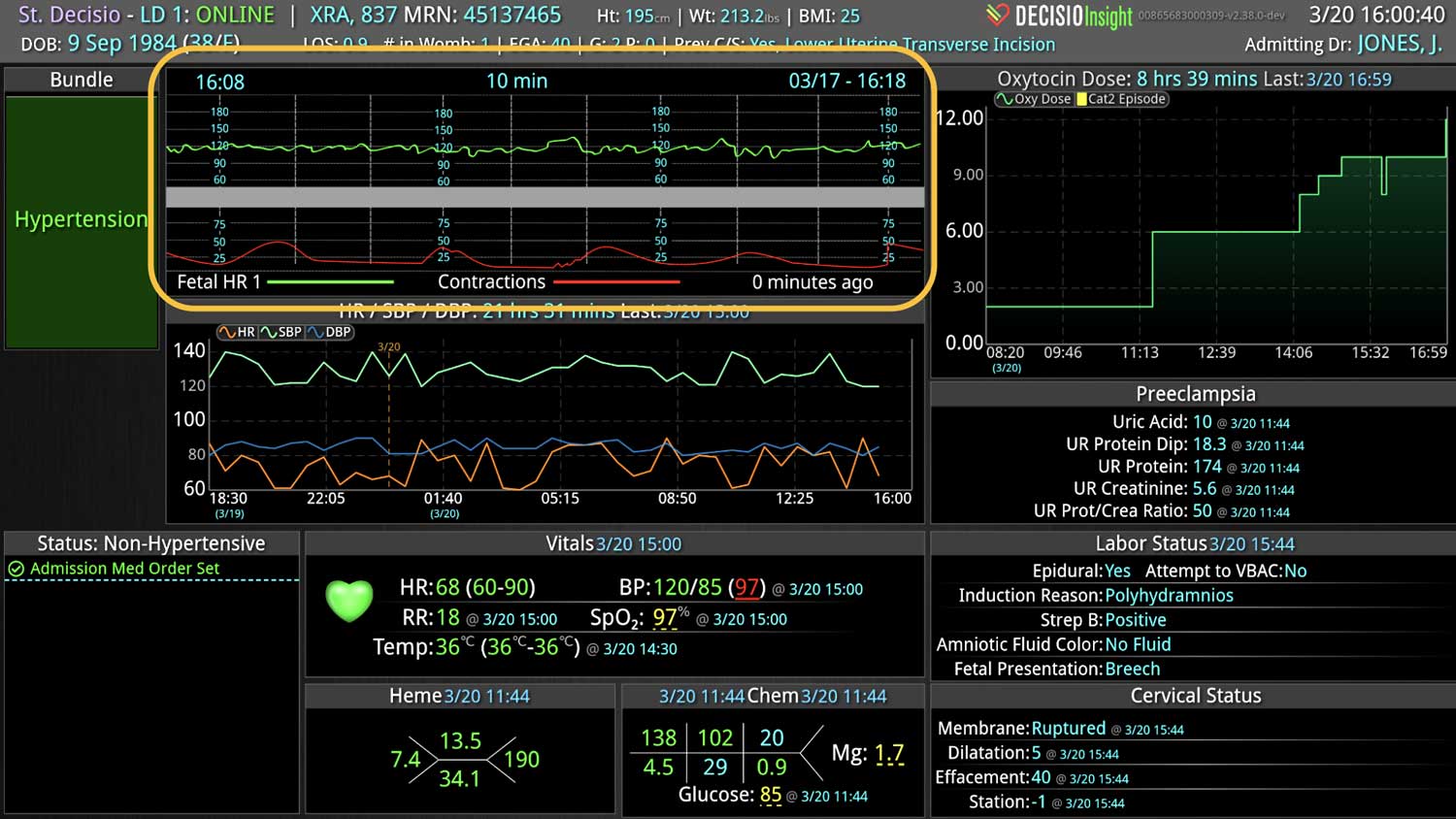
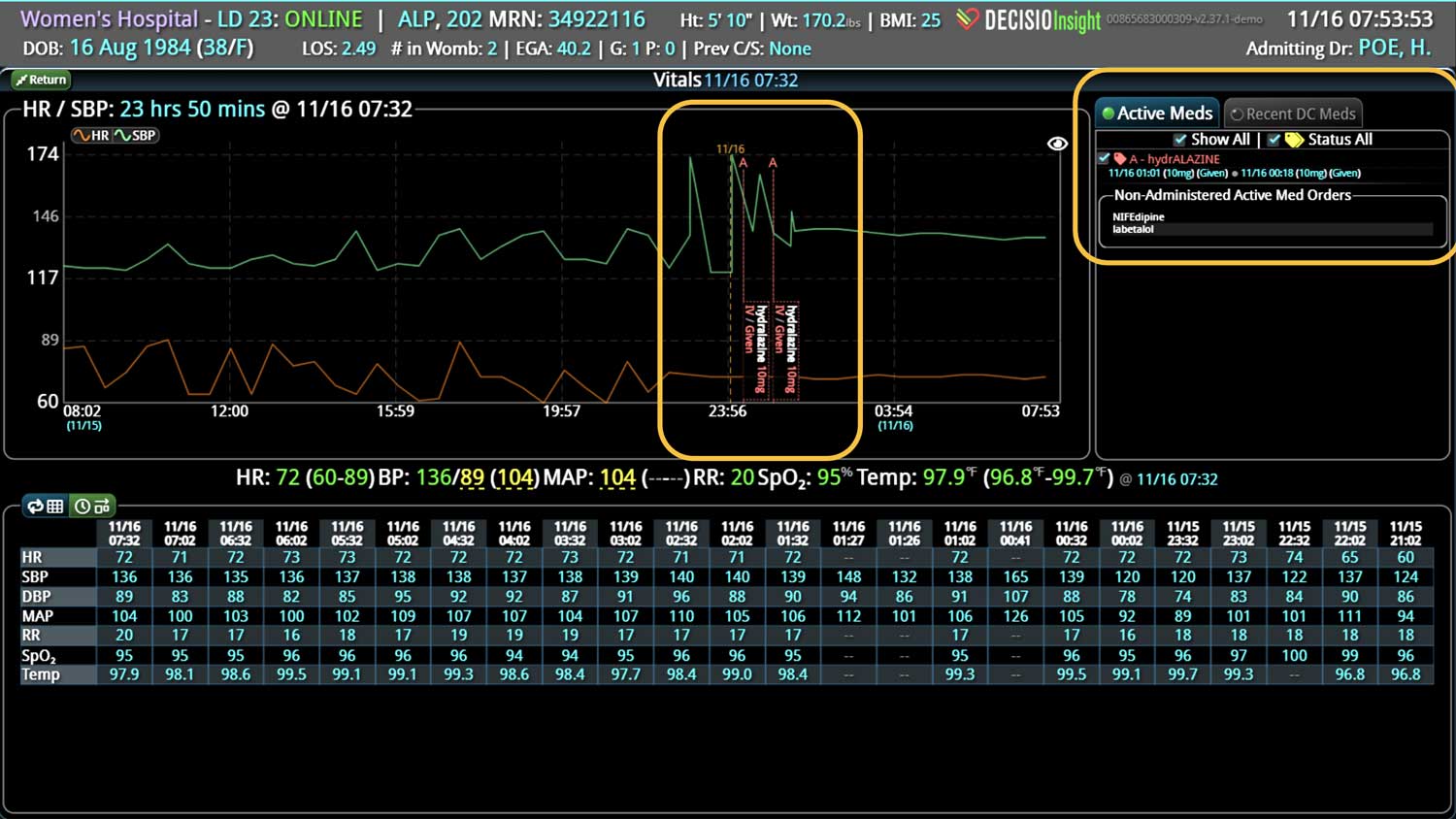
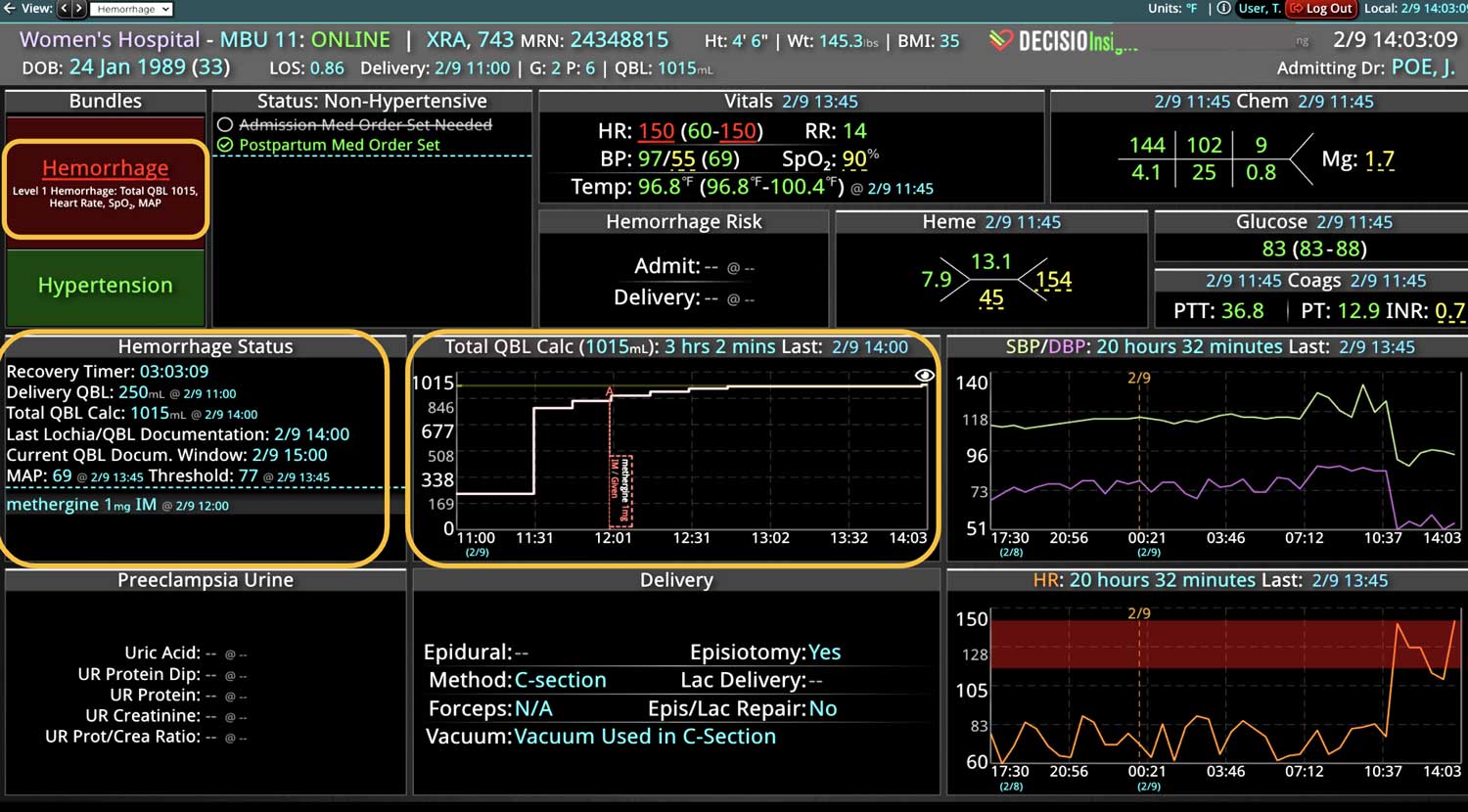
Technology for automated triggers must use all the available patient data to provide real-time, actionable notifications that are customized for the patient population. For example, medical ward patients, ED patients, and obstetric patients would require different data points from disparate data sources to be factored into their respective RRT trigger logic.
Fortunately, new RRT optimization technology enables hospitals to provide their RRT with wings so they can travel faster, further, and to more destinations. Forward-thinking hospitals are leveraging technology that provides real-time surveillance, beyond the EMR, for early intervention. Doing the right thing, 100% of the time and doing it earlier and more often is how these hospitals are leading the way to the next generation of rapid response programs.
Learn more About How we help clinicians improve patient outcomes
Schedule a call with our team to discuss how we are helping our clients revolutionize how clinicians manage patient interventions.