31 May Critical Care: Where we have been, and where are we going?
Critical Care: Where we have been, and where are we going?
Critical Care Medicine is the medical specialty of caring for patients with immediate life-threatening conditions. These types of patients need frequent assessment and have a greater need for technological support than other patients admitted to the hospital. Hence, the specialty involves the assessment and management of these critical patients in specialized units of the hospital.
As with most of the medical specialties, critical care medicine has humble origins with the development of “Iron Lung” technology during the polio epidemic in the 1950s. In the earlier days of the specialty, any physician could render Critical Care. As this area of medicine became more sophisticated – involving advanced technologies and clinical skills, specialized nursing units in the 1960s called Intensive Care Units (ICUs) were developed to care for the critically ill patients. On the training side, formalized pathways to certification, in the knowledge base and skills to care for these patients, were developed through the American Association of Critical Care Nurses. Eventually, the established medical specialties of Internal Medicine, Surgery, Anesthesiology, Emergency Medicine, and Neurology created a formal training curriculum and certification in the subspecialty of Critical Care Medicine.
ICUs and Critical Care Medicine, along with Emergency Medicine, have become the safety net of the US health care system. In the last few decades, there has been an increase in demand for critical care services. Several factors including improved life expectancy, a larger aging population, and advances in medical therapeutics have led to the increase in demand. Approximately, six million Americans, or 2% of the population, are admitted to the ICU each year, and 1 in 5 Americans receive ICU care at the end of life. Today, there are more than 80,000 adult ICU beds in the US, about 17,000 “intensivists” (MDs who specialize in Critical care), and 68,000 Critical Care nurses in the US, who care for critically ill patients. Well over 100 billion US dollars is spent annually on Critical Care, which is just over 4% of US national health care expenditures and approximately 0.72 % of the US gross domestic product and the cost of care is rising. Compounding the issue is the ongoing and increasing shortage of Critical Care trained workforce that is failing to keep up with the realities of ICU admissions and the stretching of ICU providers to deliver care throughout the entire hospital and beyond.
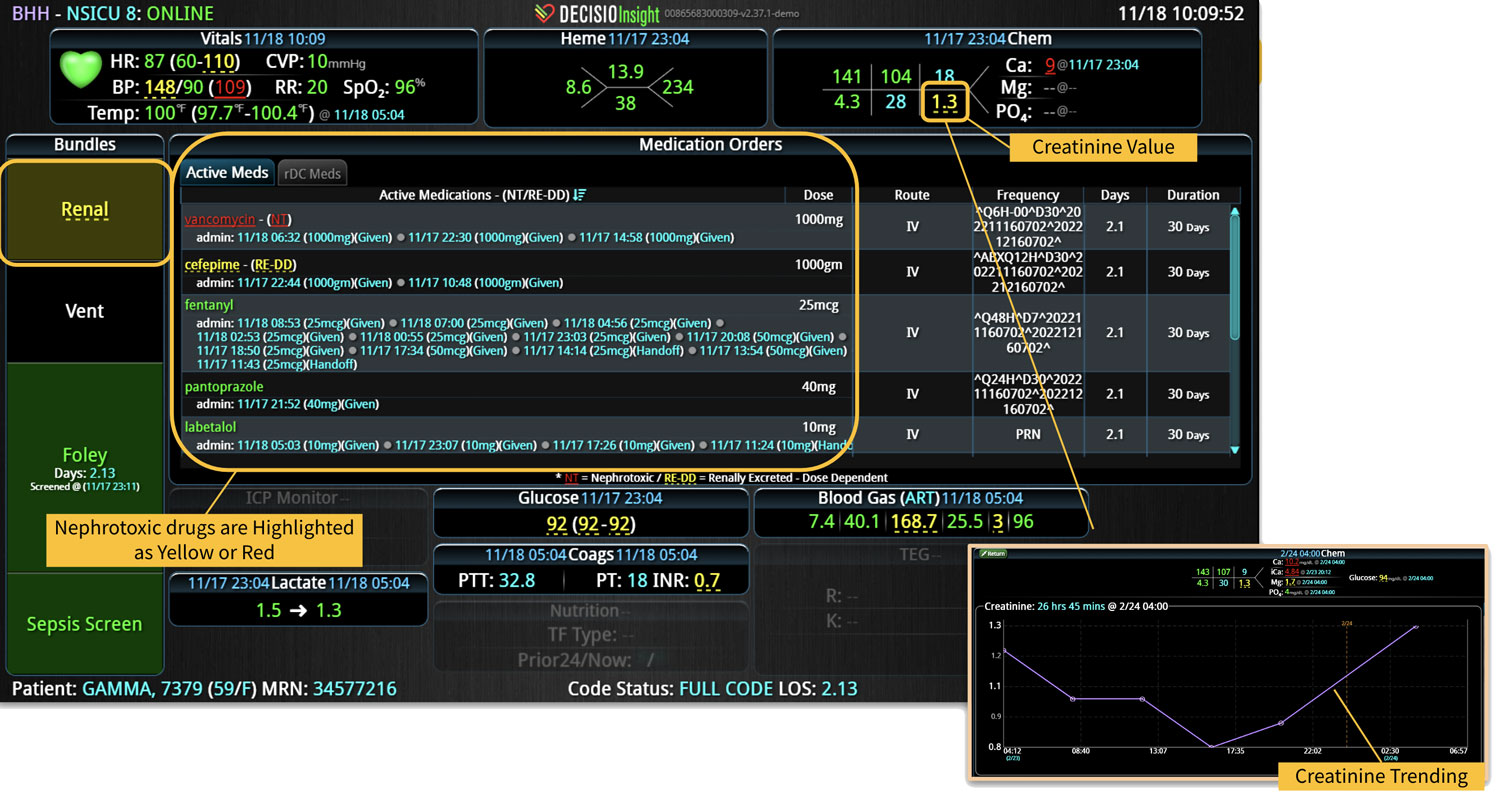
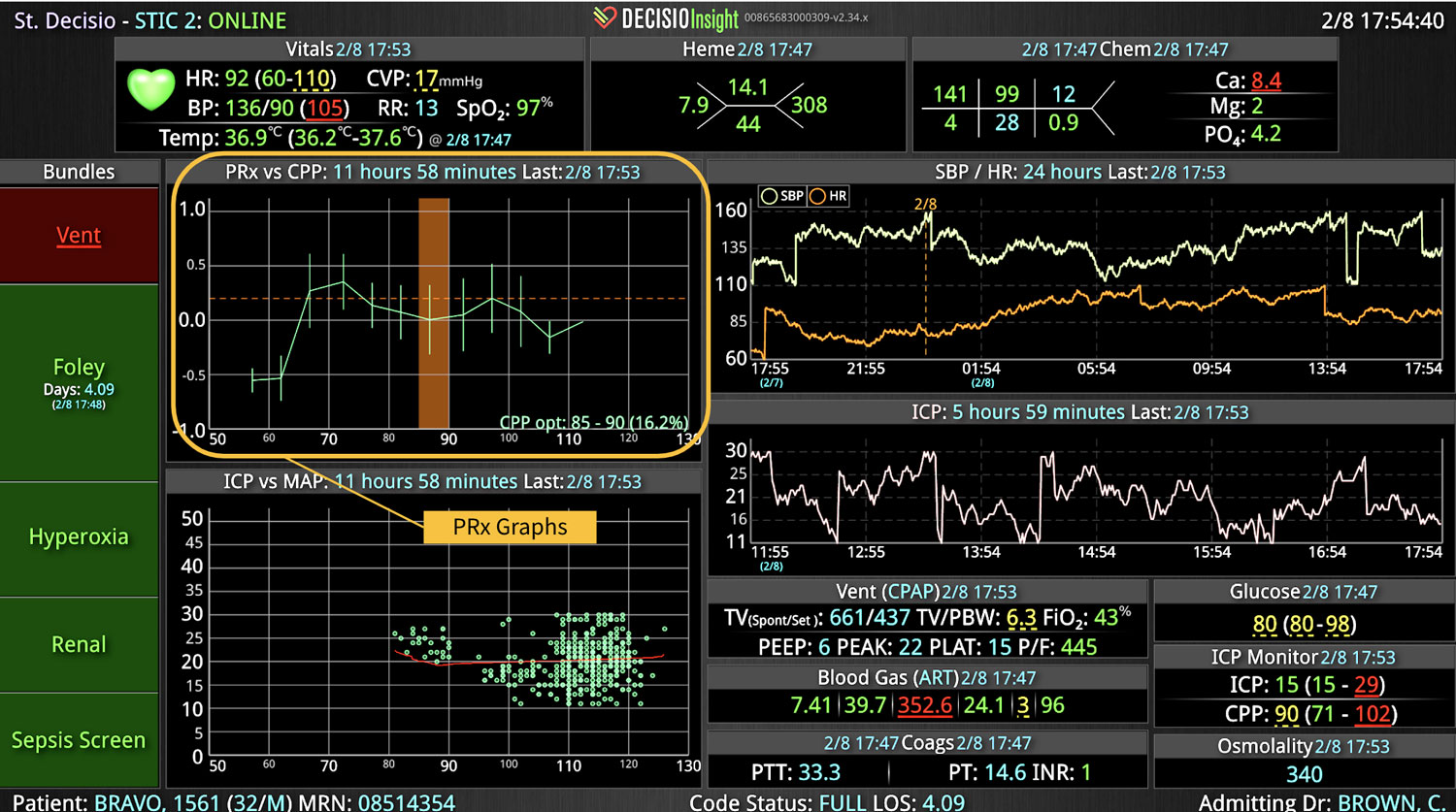
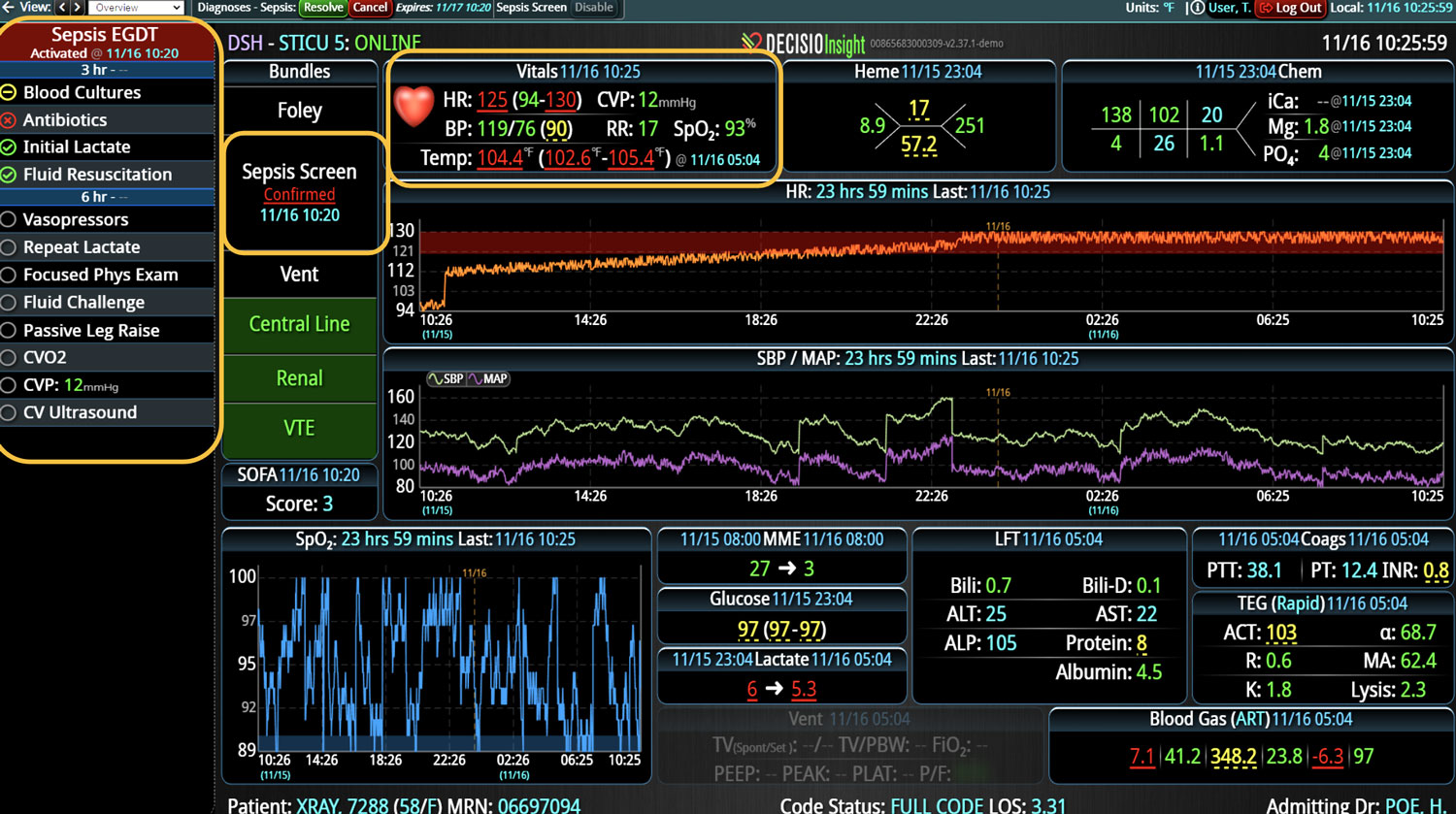
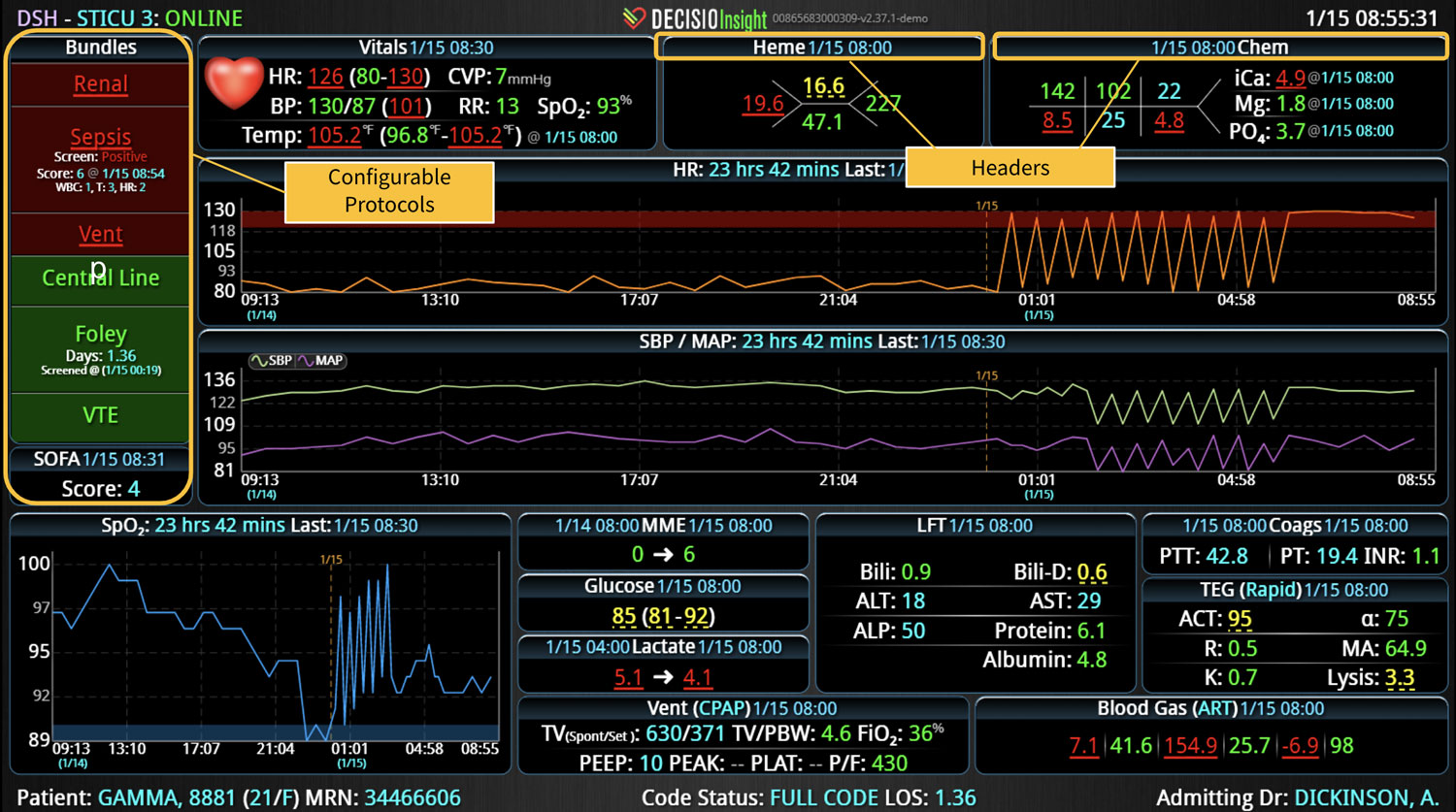
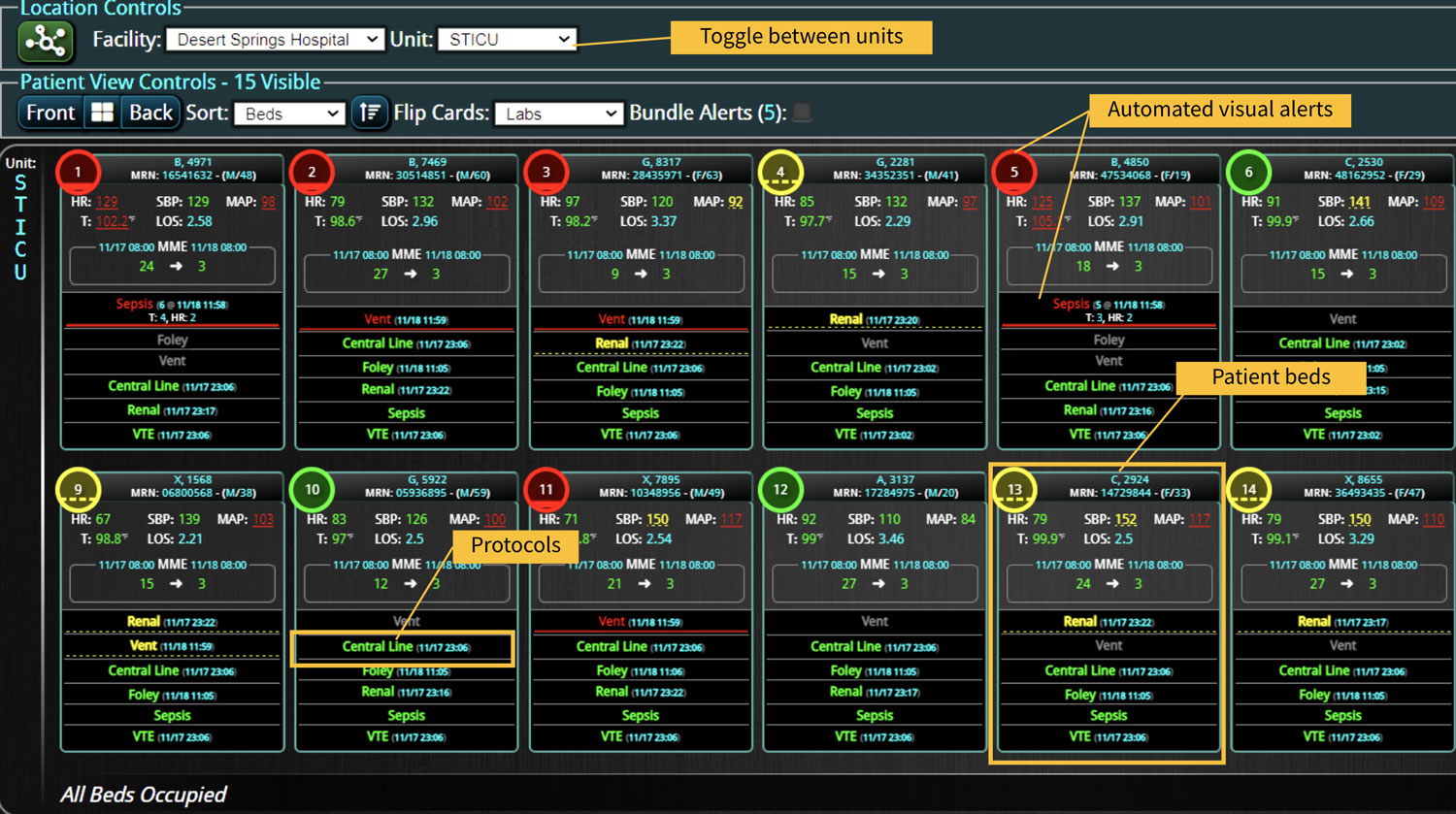
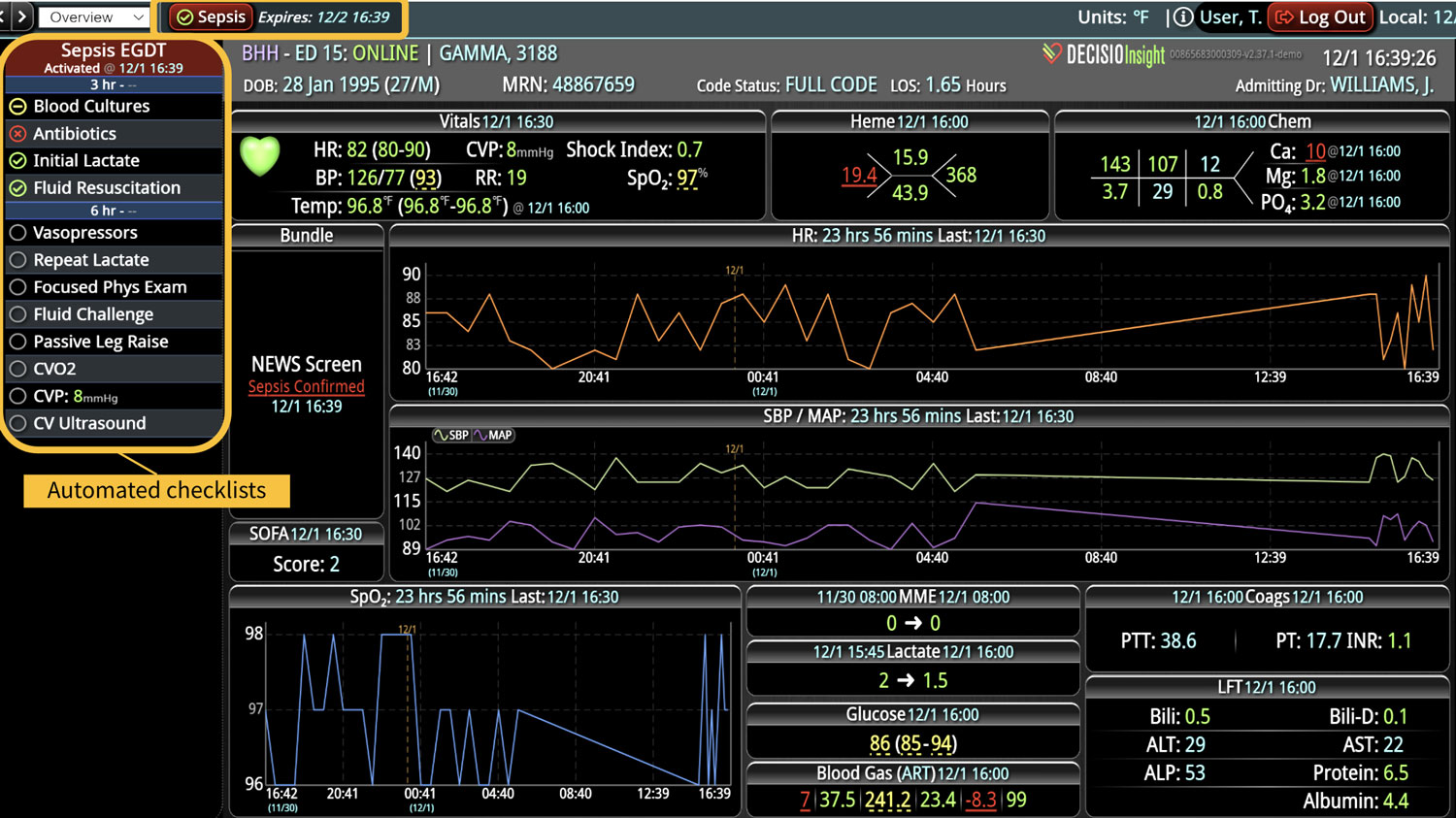
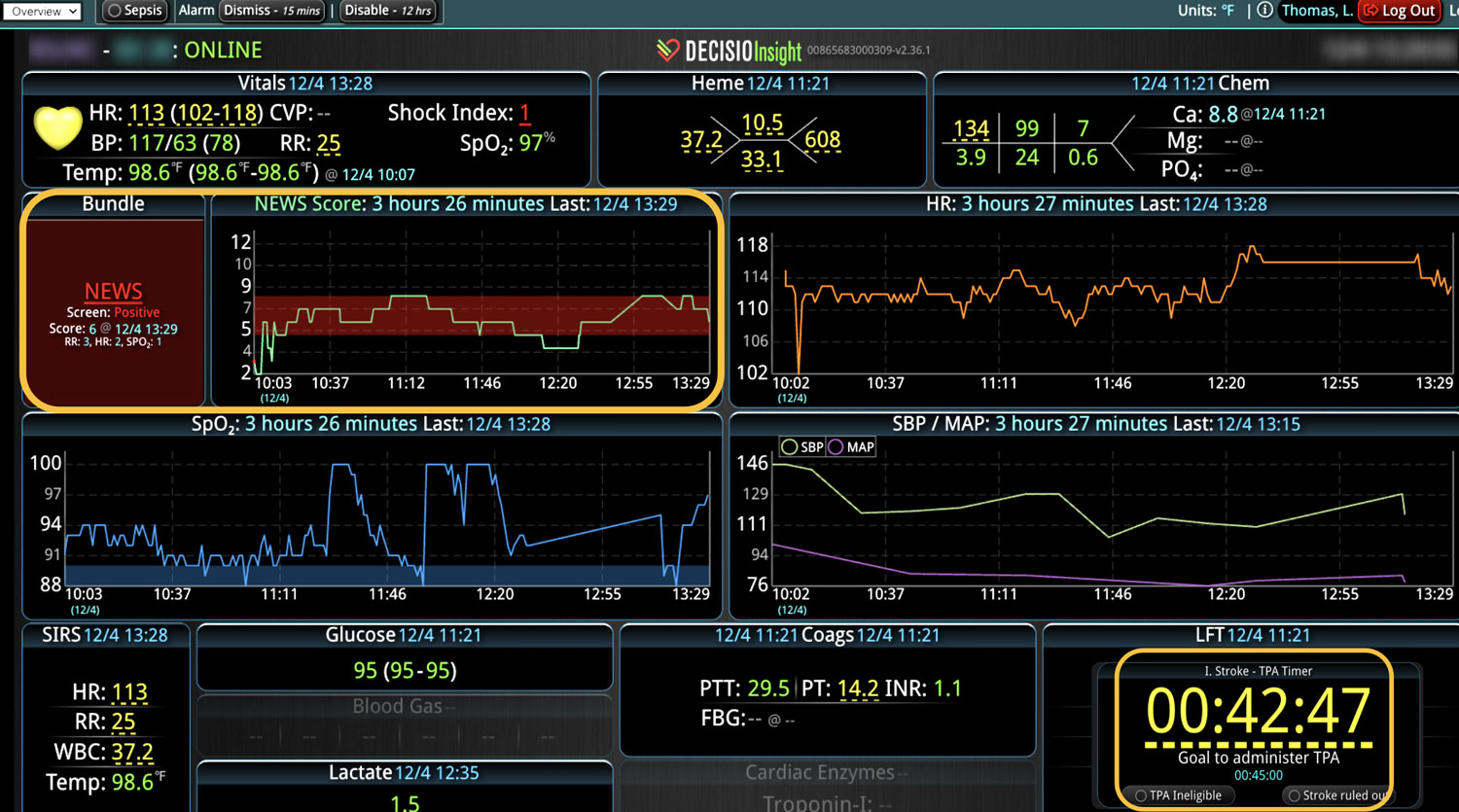
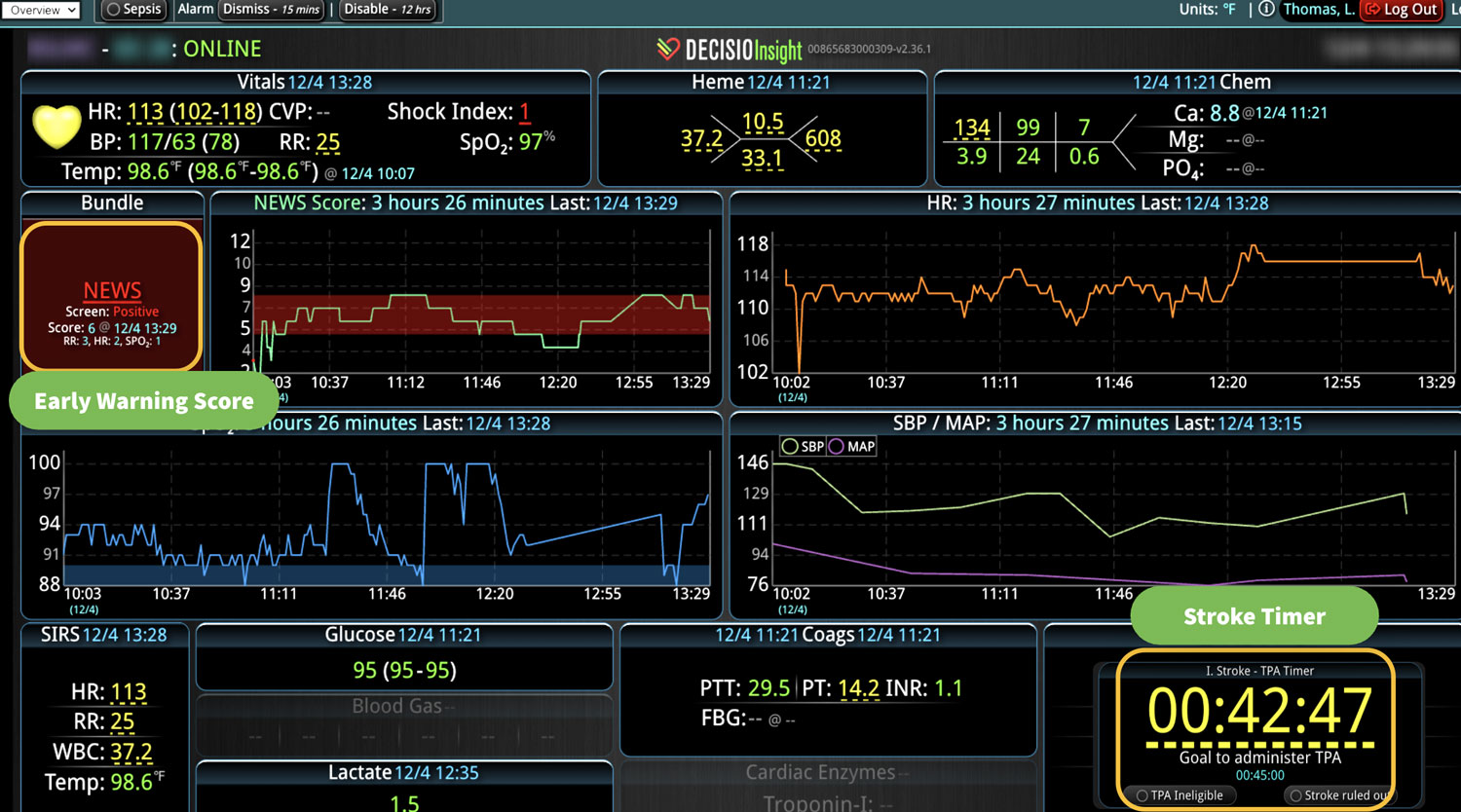
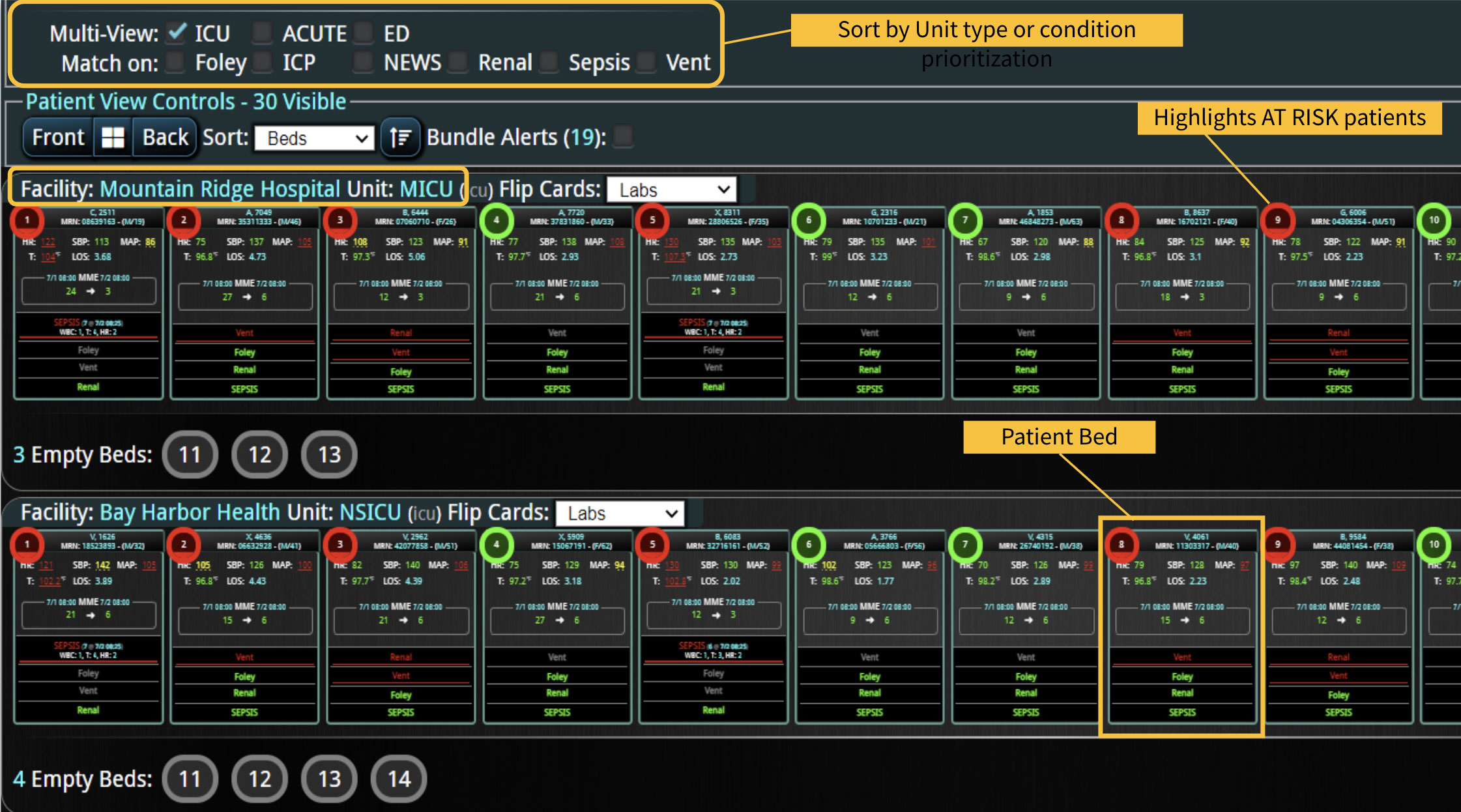
As the role of Critical Care Medicine in our health care system has expanded, so has the complexity of caring for critically ill patients. Our Critical Care system places the intensivist at the head of a large team of providers caring for individual patients. Critical care pharmacists, physical therapists, occupational therapists, respiratory therapists, nutritionists, spiritual support, case management, and, most importantly, the bedside nurses are on a typical ICU team. The intensivist receives consultative input and interventional help, usually from several medical specialists who focus on particular aspects of patient care. The intensivist incorporates these resources into a care plan while continually monitoring an extensive data set from the EHRs, bedside monitors, medication pumps, ventilators, and other medical devices to determine the patients’ progress and plot an evolving course of therapy. It has been estimated that intensivists process 1500 – 2500 data elements, per day, for each ICU patient. In addition, the evidence supporting many of the interventions performed in the ICU is scarce, and practice variability is abundant.
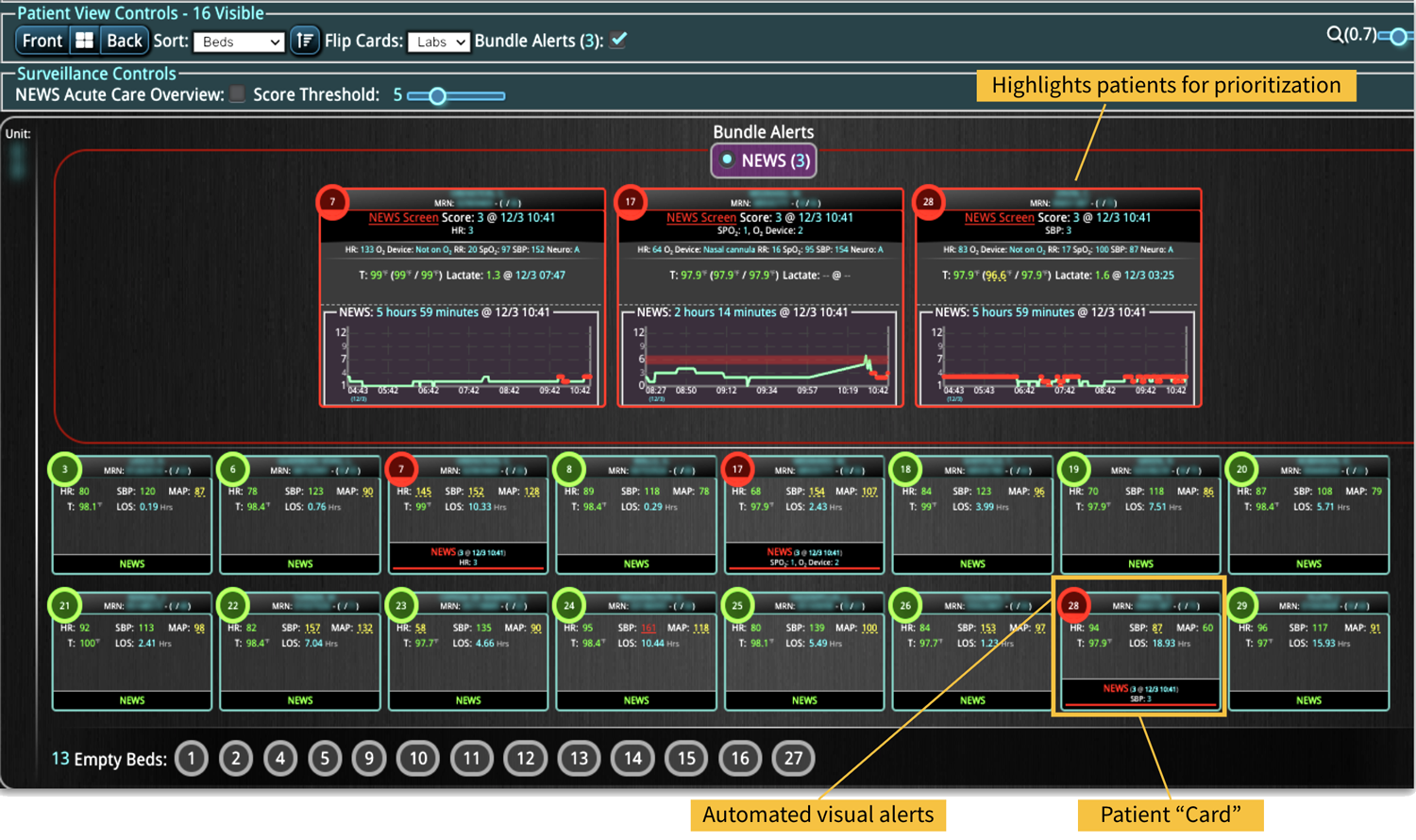
With the complexity of ICU patients, their typical dynamic conditions, and all the data inputs required to optimize their care, it is no wonder that ICUs are care environments where Intensivists would benefit from tools that help them process data into useful signals to warn against potential detrimental events or opportunities to intervene in a timely fashion. Large quantities of clinical data could be analyzed by computational systems and served to the bedside clinicians in the form of manageable, interpretable, and actionable knowledge that augment the clinician’s decision-making capacity. False alerts have to be kept to a minimum and systems have to be continuously improved through a collaborative and scientifically rigorous approach. Data-driven systems and clinicians have to work hand-in-hand to provide the “right care at the right time,” to quote the Society of Critical Care Medicine slogan. This “decision support” practice will be a key to the evolution of Critical Care practice going forward and will make an enormous impact on the quality and safety of care for our most vulnerable patients, the critically ill patient.
J Pat Herlihy, MD
Professor, Baylor College of Medicine.
Chief, Critical Care Service, Baylor St. Luke’s Medical Center
Texas Medical Center, Houston, TX
Learn more About How we help clinicians improve patient outcomes
Schedule a call with our team to discuss how we are helping our clients revolutionize how clinicians manage patient interventions.