09 Aug Hospital Acquired Conditions Reduction Program: May the Odds Be Forever in Your Favor
Hospital Acquired Conditions Reduction Program: May the Odds Be Forever in Your Favor
Unfortunately, we see the following scenario play out all too often: A family brings an elderly loved one to the hospital for what was intended to be a simple procedure. While hospitalized, she develops a urinary tract hospital-acquired condition (HAC) from foley catheter complications. The family was prepared for a simple stay, and instead they are faced with a prolonged hospitalization with risks of bacteremia and sepsis.
A colleague once wrote that she sees HACs like an eccentric family member with a habit of showing up unannounced, luggage in tow. He brings suitcases full of complications and leaves a trail of havoc in his wake. Simply stated, this pesky relative created a potentially avoidable disruption – he could have simply called ahead! In the same vein, HACs are avoidable complications that occur while a patient is hospitalized for an unrelated condition.
Trends in HACs
In 2014, the CDC estimated that on any given day, 1 in 25 hospitalized patients would develop at least one infectious HAC. Despite this seemingly high statistic, HACs are decreasing. Between 2008 and 2014, we have seen:
· A 50% decrease in central line-associated bloodstream infection
· A 17% decrease in surgical site infection after abdominal hysterectomy
· A 13% decrease in hospital-onset MRSA blood infection
· An 8% decrease in C. difficile infection.
Introducing the Hospital Acquired Condition Reduction Program (HACRP)
Now picture the moment when you and your spouse have a heart-to-heart about the frequent, unsolicited visits by Uncle “Bob.” It’s true, that since 2008, his visits have decreased, but the moment has arrived to attempt a rational conversation with the uncle, otherwise his unannounced and unwanted visits may never cease.
Similarly, the HACRP was implemented in 2015 under the Patient Protection and Affordable Care Act (ACA). This “conversation” between CMS and hospitals was intended to further reduce HACs by tying them to reimbursement. A model was implemented whereby hospitals performing below the national HAC performance score would face a 1% penalty in CMS reimbursement.
What does HACRP evaluate?
HACRP only measures a subgroup of HACs divided into two domains. Domain 1 includes predominantly non-infectious complications such as pressure ulcers, pneumothorax, and DVTs.
Domain 2 includes five infectious HACs:
· CLABSI – Central Line-Associated Bloodstream Infection (CLABSI)
· CAUTI – Catheter-Associated Urinary Tract Infection (CAUTI)
· SSI- Surgical Site Infection of colon and hysterectomy
· MRSA Methicillin-resistant Staphylococcus aureus bacteremia
· CDI – Clostridium difficile Infection
Seeing the light…
After the uncomfortable and failed attempt to reason with Uncle Bob, you pull out the one card that almost always works: ignite some competition. You say: “Well, it’s just that Aunt Betsie and Uncle Bernie always let us know when they’re coming, and we are able to plan for their visit and spend quality time with them.” The hope is that competition will motivate Uncle Bob.
Similarly, the HACRP introduced the competition card with the HACRP by “grading” hospitals against each other. Hospitals must work harder and harder to keep their HAC score low enough to prevent a 1% penalty. Much like the family’s attempt with Uncle Bob, the hope was that CMS would move the needle on HACs by creating a sense of competition.
Survey says…
In 2017, a reported 769 of 3,203 hospitals who ranked in the worst performing quartile will face the 1% penalty in 2017. This is compared to 751 hospitals out of 3,211 hospitals penalized in 2016. Not quite the results we were expecting…
HACRP, with its huge penalties totaling $364M last year, is coming under scrutiny in the year end, as clinicians question the validity of their calculations – considering the underwhelming outcome in HACs reduction. In a recently published study, data shows that large hospitals are more likely to be identified as poor performers for measures that have a very low probability of complications.
The bottom line
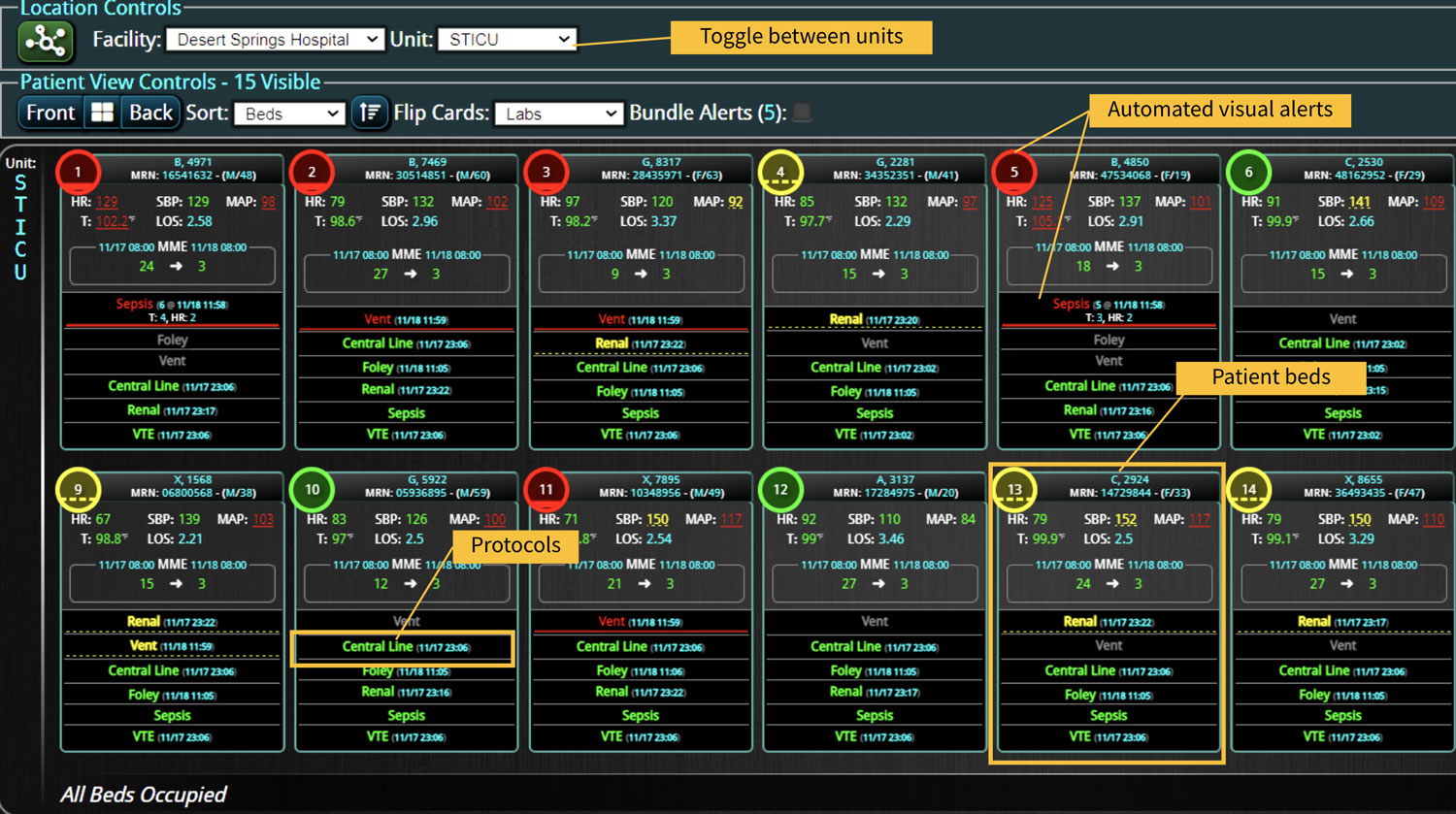
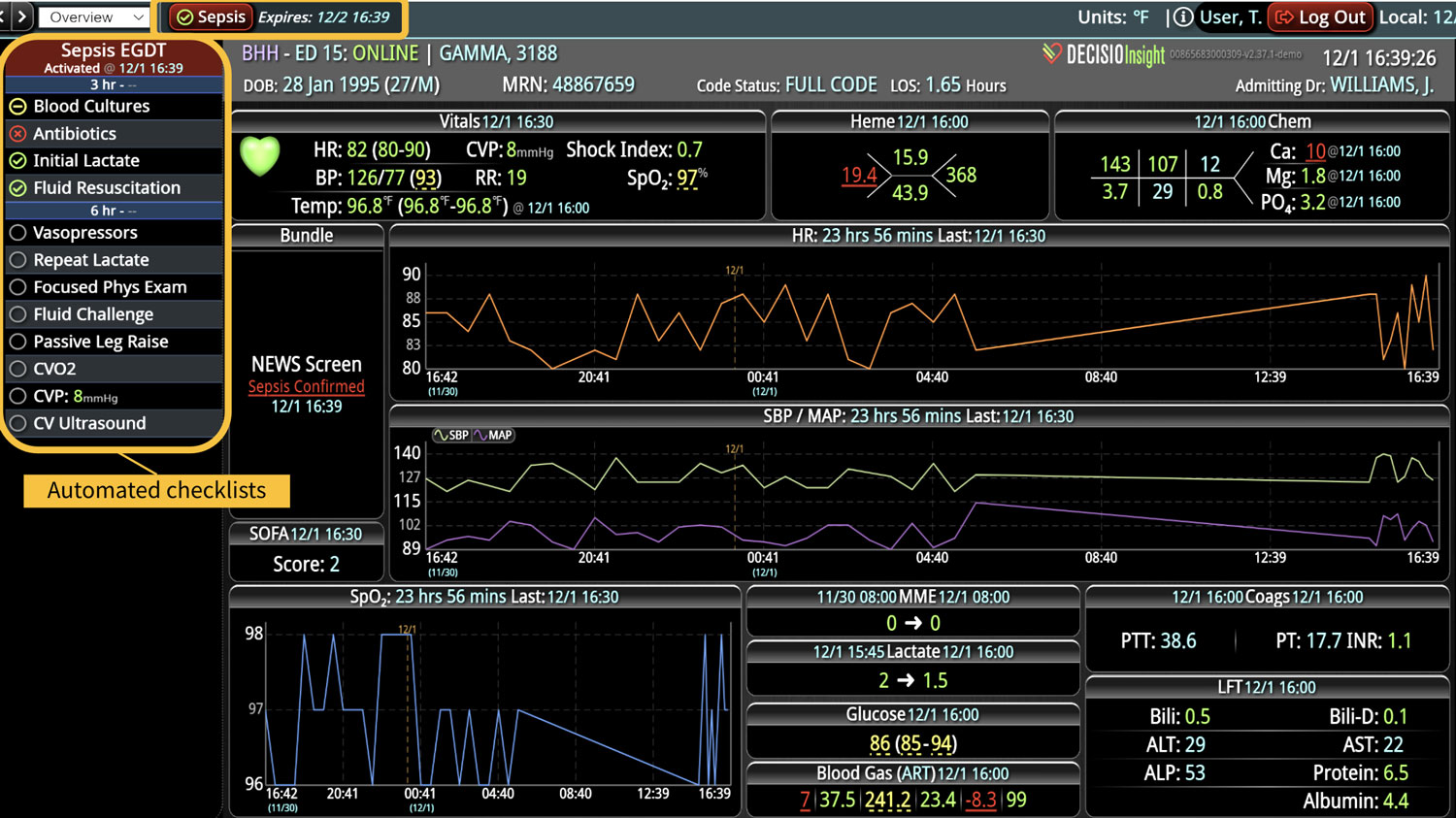
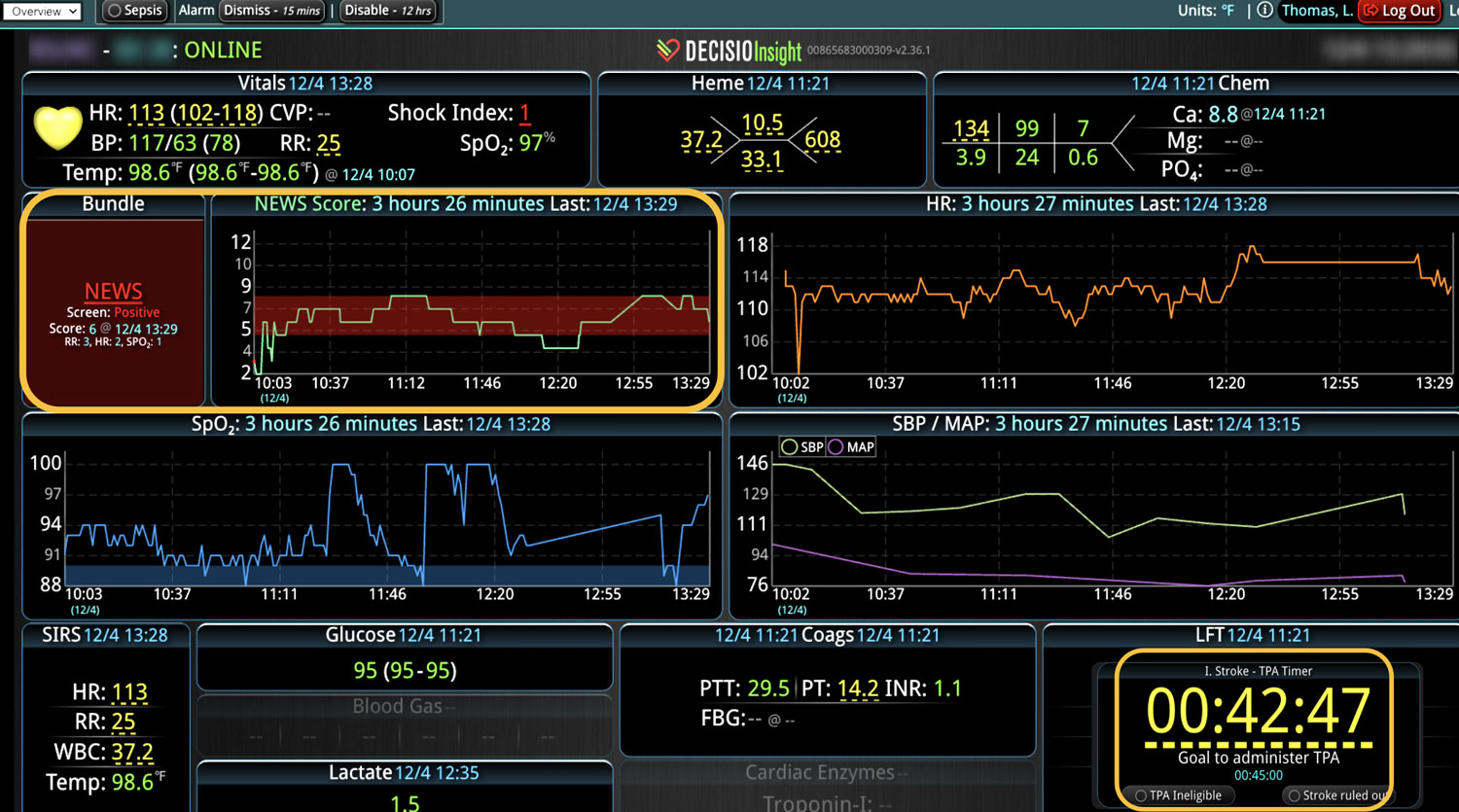
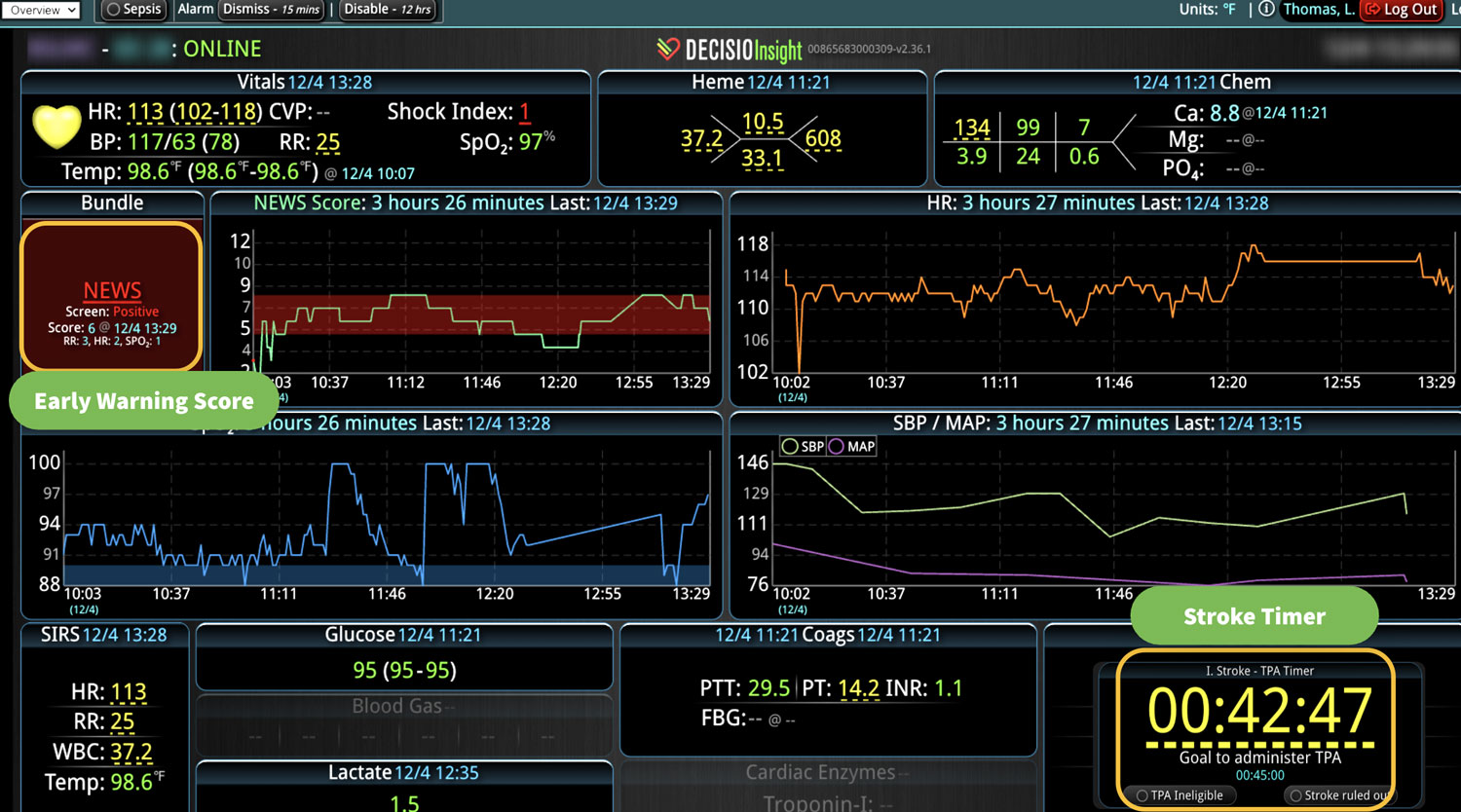
Now more than ever, hospitals are struggling to find ways to pull ahead of the curve and stay penalty-free. Tools are currently available to hospitals that make this goal achievable. “Clinical Decision Support” (CDS) is no longer the one-size-fits-all order sets introduced almost 20 years ago.
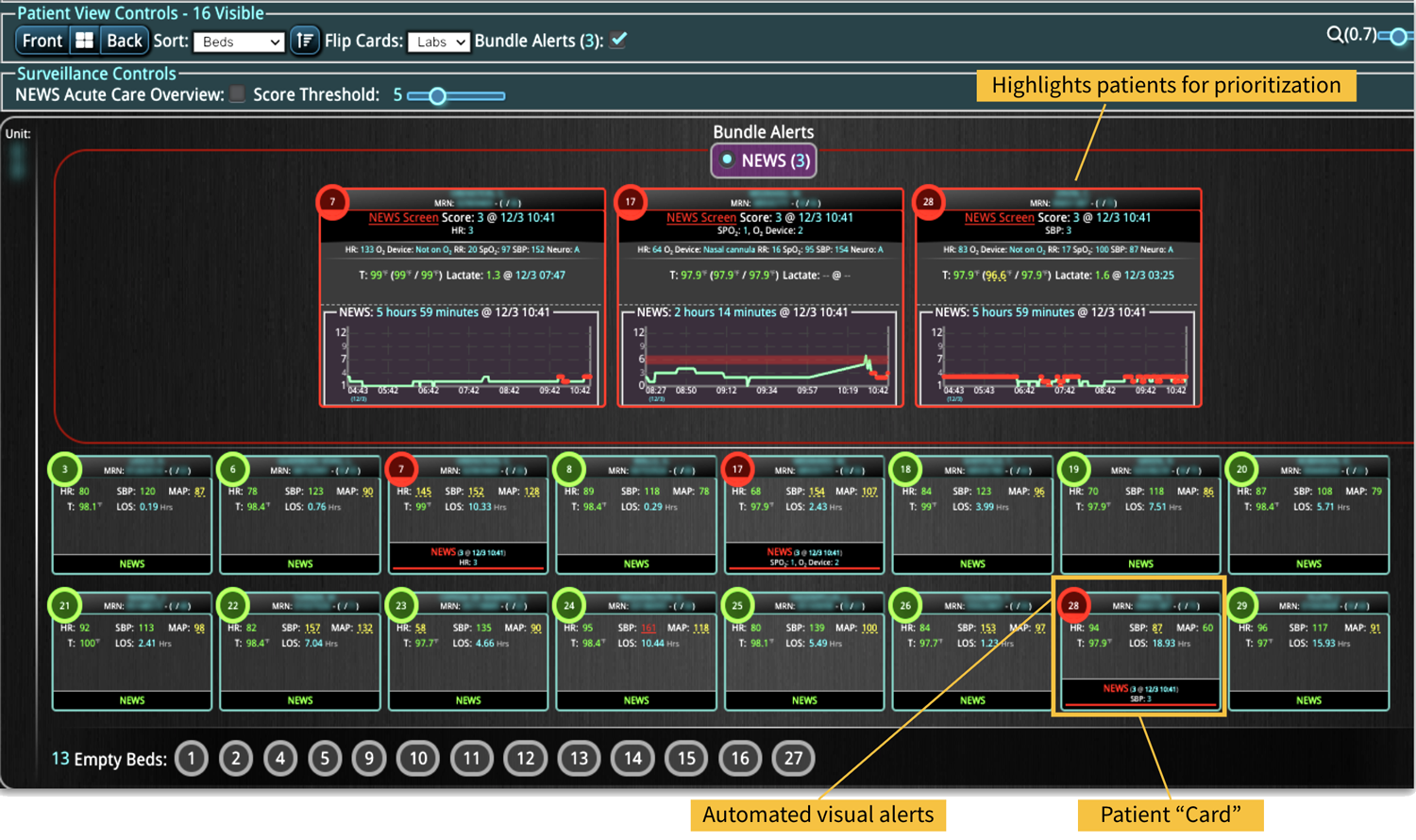
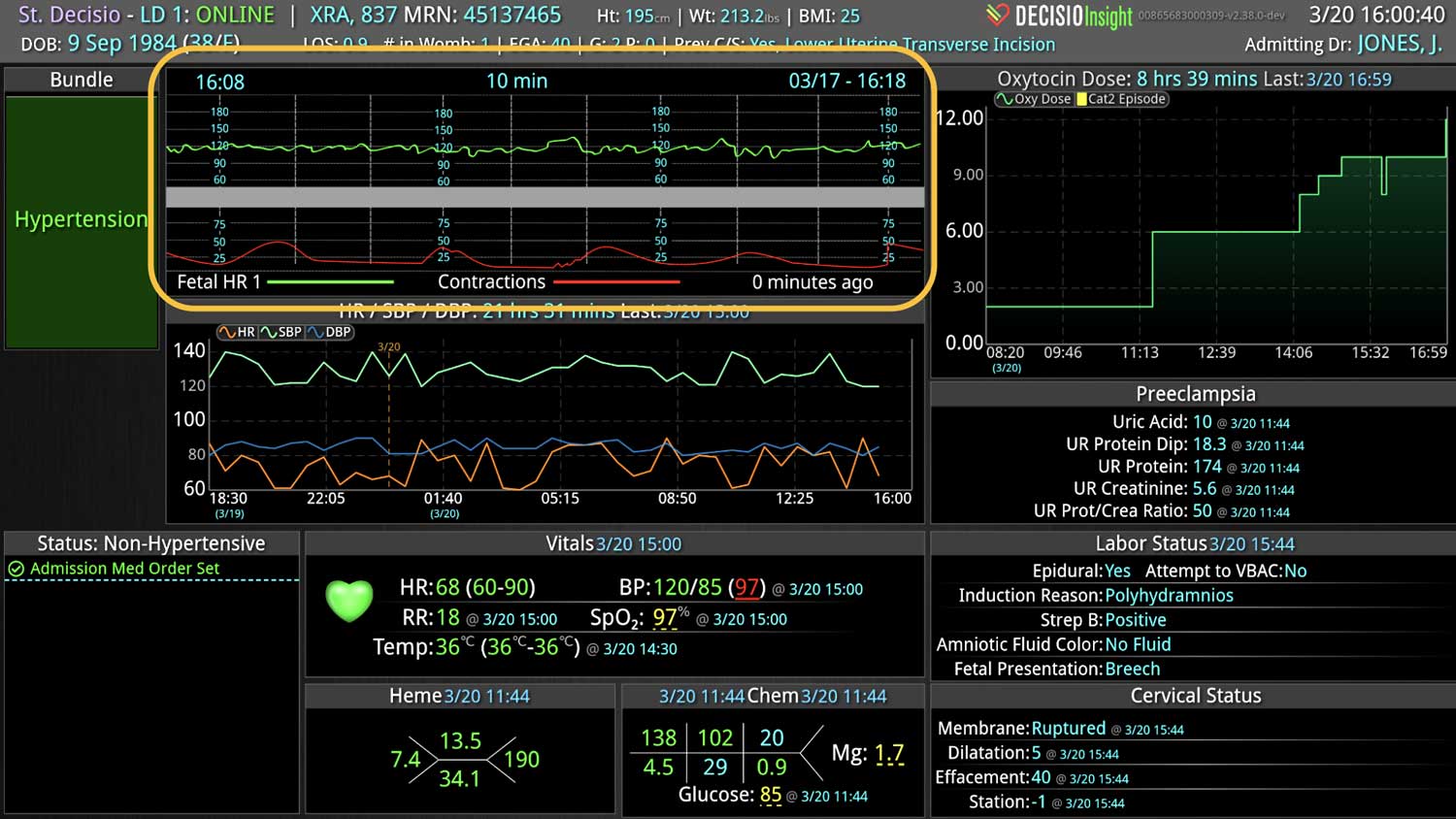
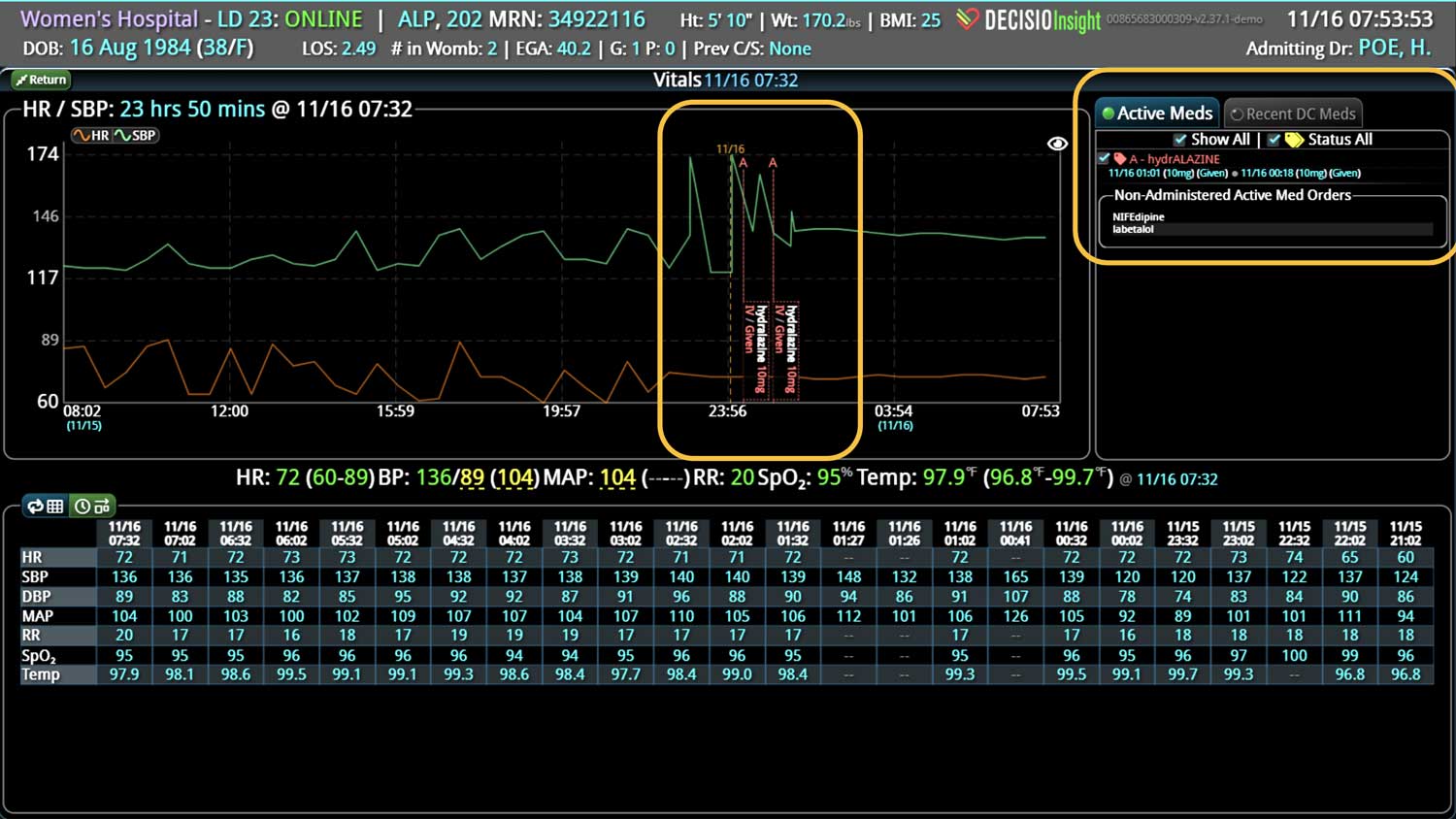
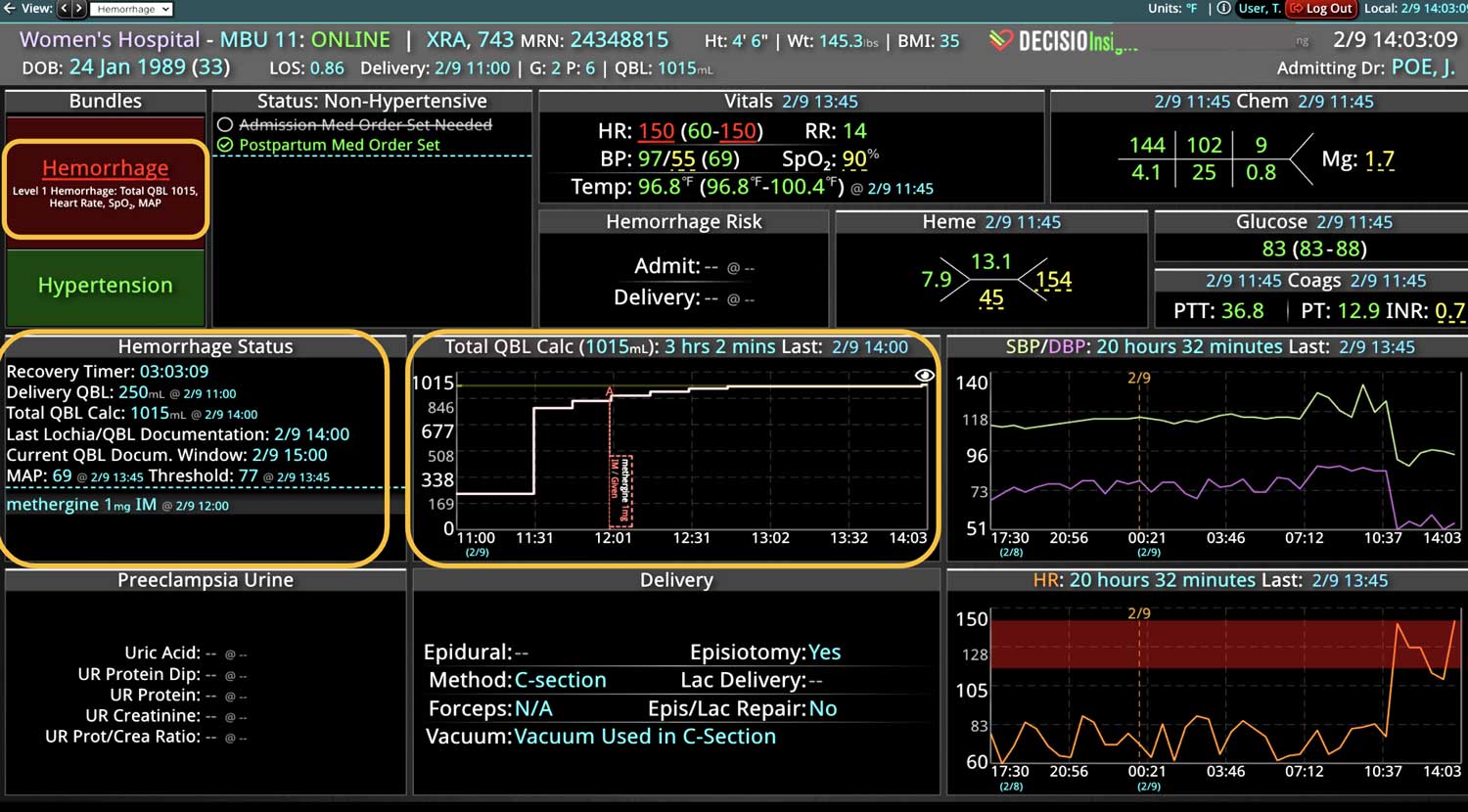
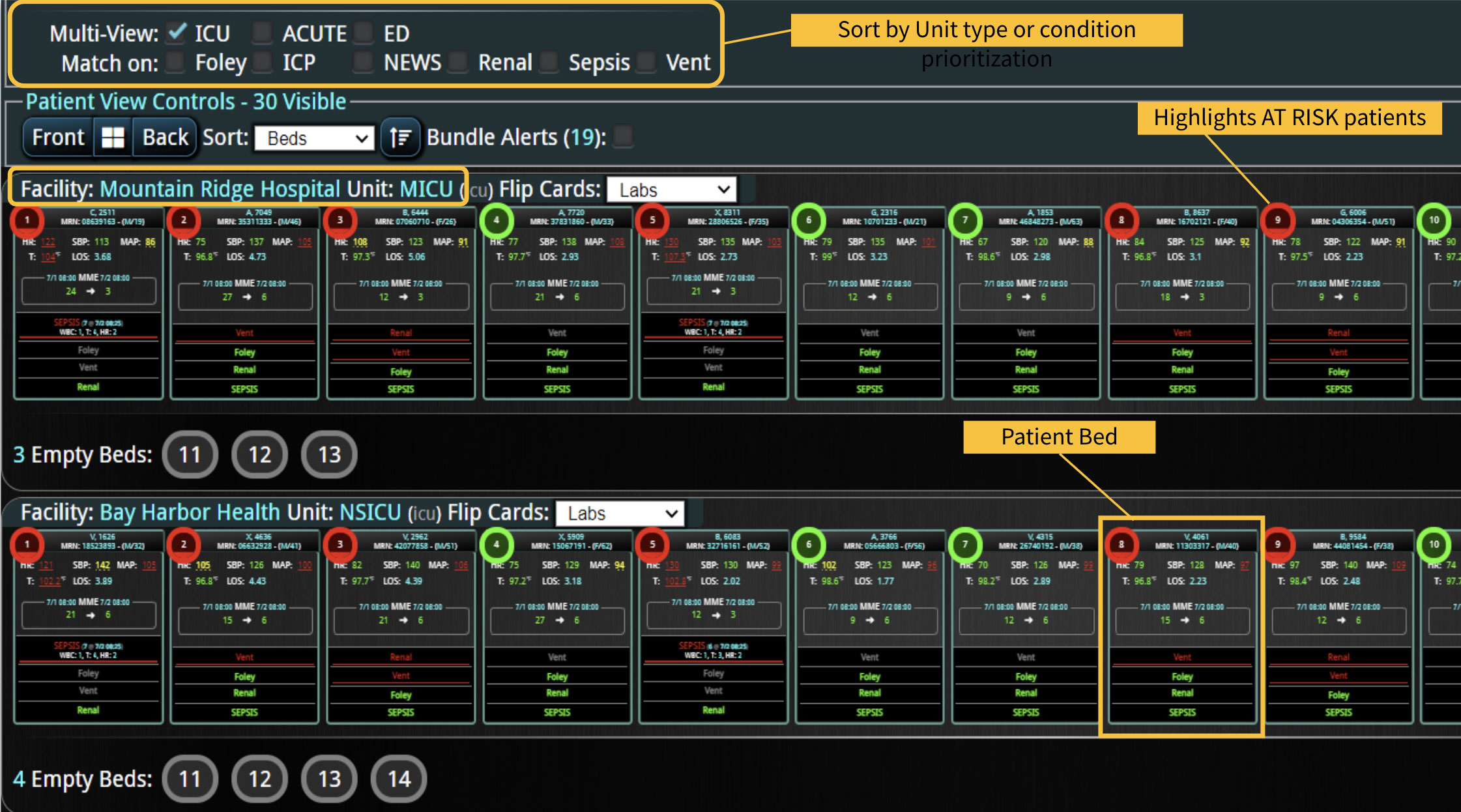
Today, physicians can use real time detection of HACs before they happen, using patient-specific CDS tools that alert the care team of a change in a patient’s condition that indicates a HAC is looming around the corner.
So, maybe the attempt at rational pleading with your pesky uncle was unsuccessful. And maybe attempts at igniting competition by pointing out how more considerate relatives call ahead fell on deaf ears. But maybe putting a “Find My Friends” app on Uncle Bob’s phone, with an automated notification when he’s approaching might be the solution you’re looking for.
Similarly, maybe the answer isn’t sending hospitals into a battlefield with a simple blessing like: “Happy HACRP Games! May the odds be forever in your favor.” Rather, maybe arming them with the right equipment to predict, prevent, and rapidly respond to risks of HACs, instead, is a better strategy.
Learn more About How we help clinicians improve patient outcomes
Schedule a call with our team to discuss how we are helping our clients revolutionize how clinicians manage patient interventions.