08 May Patient and family-centered care: transforming care delivery in the intensive care unit
Patient and family-centered care: transforming care delivery in the intensive care unit
Patient and family-centered care (PFCC) has become an integral component of modern medicine. It is widely adopted in outpatient care settings, where it is improving the quality and efficiency of care while increasing patient and provider satisfaction. Additionally, CMS payment models, such as MACRA, are furthering adoption by tying physician payment to patient and caregiver experience and patient-reported outcomes.
But how has PFCC fared in the intensive care unit (ICU)? In the ICU, emotions are heightened, decision making is rapid, family member involvement is high, and the risk of death is always looming. These challenges have contributed to slower adoption of PFCC in the ICU. Healthcare providers have traditionally been viewed as a risk-averse group with slow cultural transformation and resistance to workflow changes – particularly those directly affect care delivery. However, these behavior patterns are changing – even in the ICU.
Shifting the paradigm
More and more ICUs are now embracing PFCC. Traditional ICU environments are increasingly viewed as outdated and obstructive. It wasn’t that long ago that visitation periods only occurred twice daily, and physicians could round on a patient for days without ever meeting a family member. Status updates were shared with families only by nurses who had to piece together data from several sources to do so, and families frequently learned of care decisions after they had been made. These barriers impeded trust-building and had potentially harmful emotional and physical effects on patients and their families.
Today, more and more ICUs are incorporating various degrees of PFCC. The initial step for a PFCC model is typically the establishment of a multidisciplinary team including an attending physician, nurses, social workers, technicians, anesthesiologists, pharmacists, rehab therapists, and others involved in a patient’s care plan. This truly creates a care “team” – whereby everyone has an equal voice. Once this foundation is put in place, patient and family members are added to the team. Workflows including family-centered rounds and multidisciplinary family conferences are implemented. Many ICUs have also created programs such as advisory boards comprised of former patients who contribute to the development of programs and policies.
The heart of patient and family-centered care: the ICU nurse
To patients and families, the ICU nurse is their trusted advisor, care provider, educator, and counselor. He or she is whom they first turn to for answers and assurances. However, despite the large emotional and clinical responsibility placed on these nurse champions, very few have adequate support in the form of PFCC protocols or guidelines. ICU nurses are on the front lines of PFCC but aren’t provided with the support they need for addressing complex treatment questions, managing family disagreements, or even choosing which care activities are safe for family members to perform.
The lack of standardized workflows additionally fuel the anxiety among many ICU nurses that PFCC will consume a significant portion of their limited time. However, when properly implemented, PFCC in the ICU can measurably save clinician time and enable top-of-license work for nurses and the rest of the care team by proactively addressing patient and family concerns. Shared knowledge reduces lengthy family conferences, role confusion, and repetition of previously answered questions.
Empowering the nurse champion
To assist ICU nurses in providing PFCC, hospitals are beginning to provide evidence-based protocols, standardized workflows, guidelines for escalation of support, and educational materials to share with families.
Some forward-thinking hospitals, including a cohort of four large university hospitals, are even developing digital learning libraries. Digital tools centralize information to make it more easily accessible for patient and families. But maintaining relevant, up-to-date content is a large undertaking. Most hospitals are still searching for provider-facing clinical tools that enable rapid, patient-specific care interventions. Thus, additionally implementing family-facing digital tools is a daunting, if not unmanageable, undertaking.
The best of both worlds
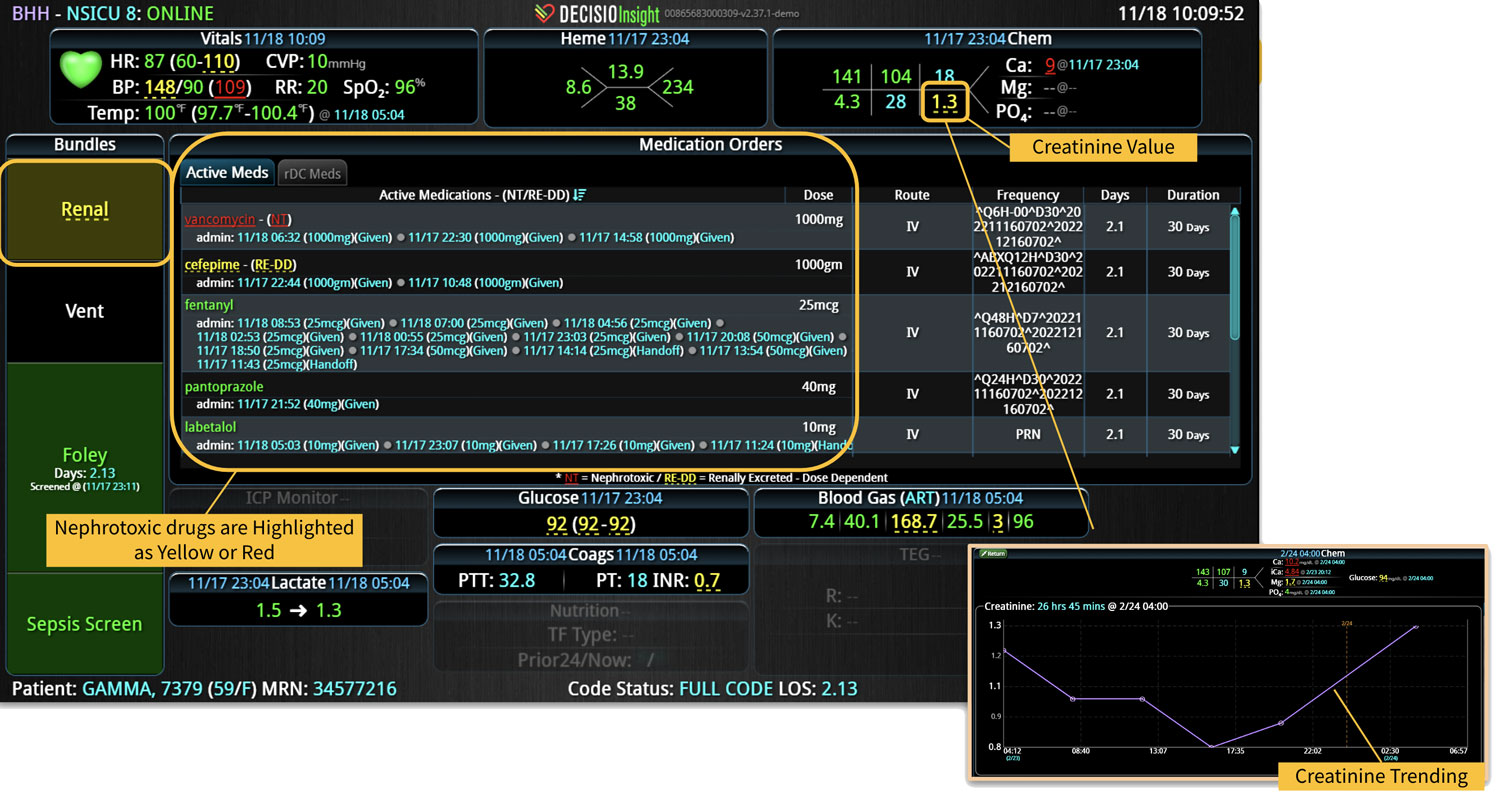
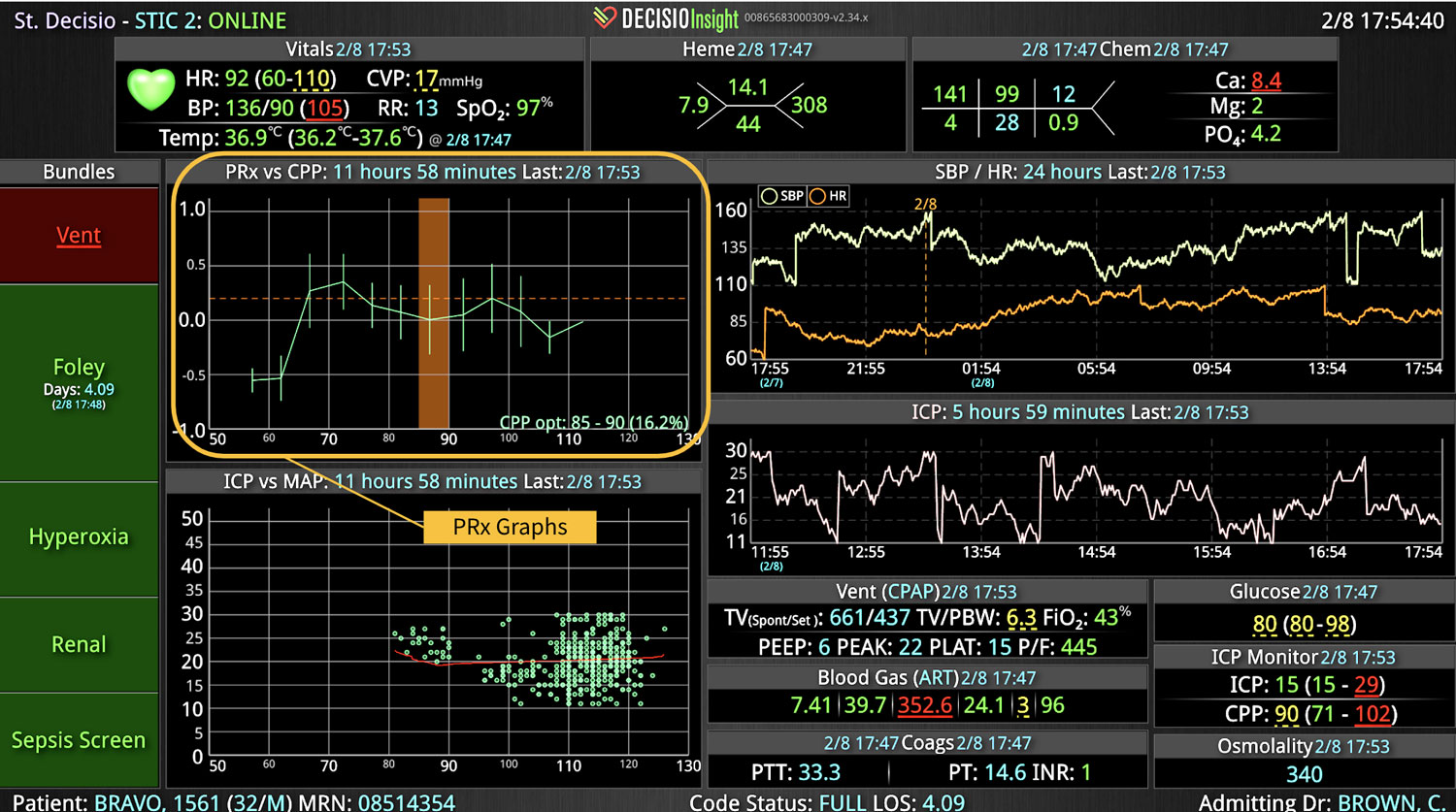
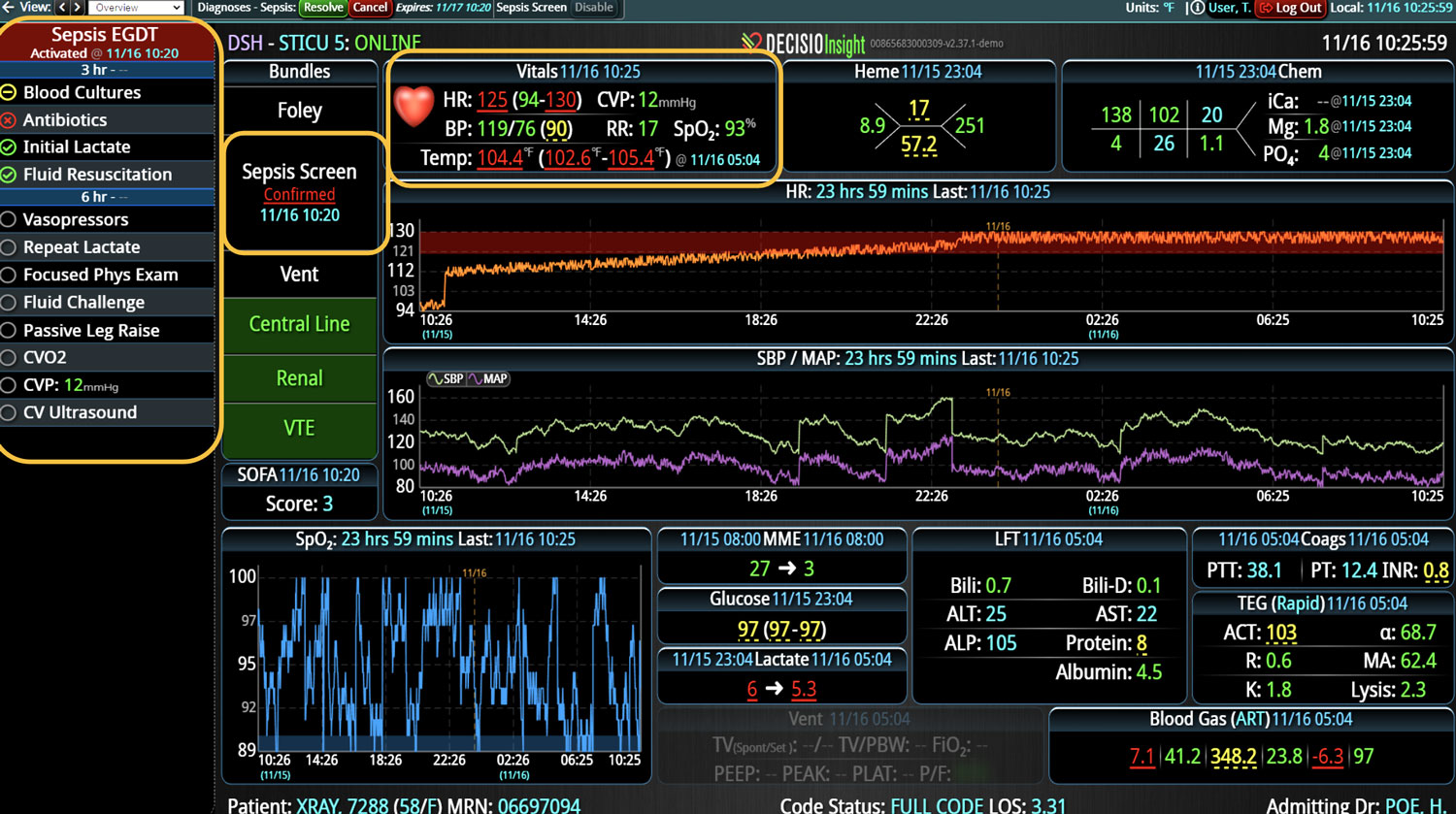
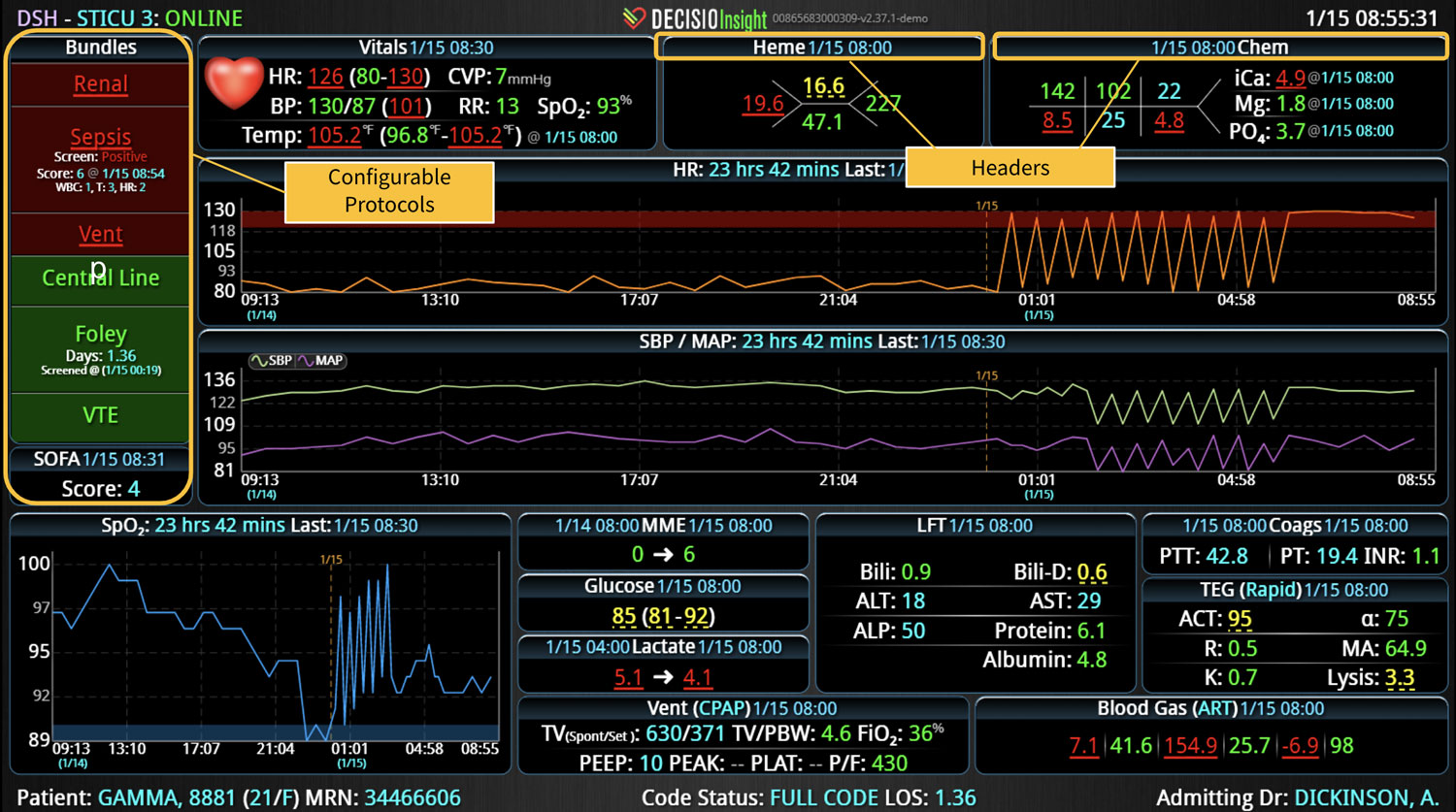
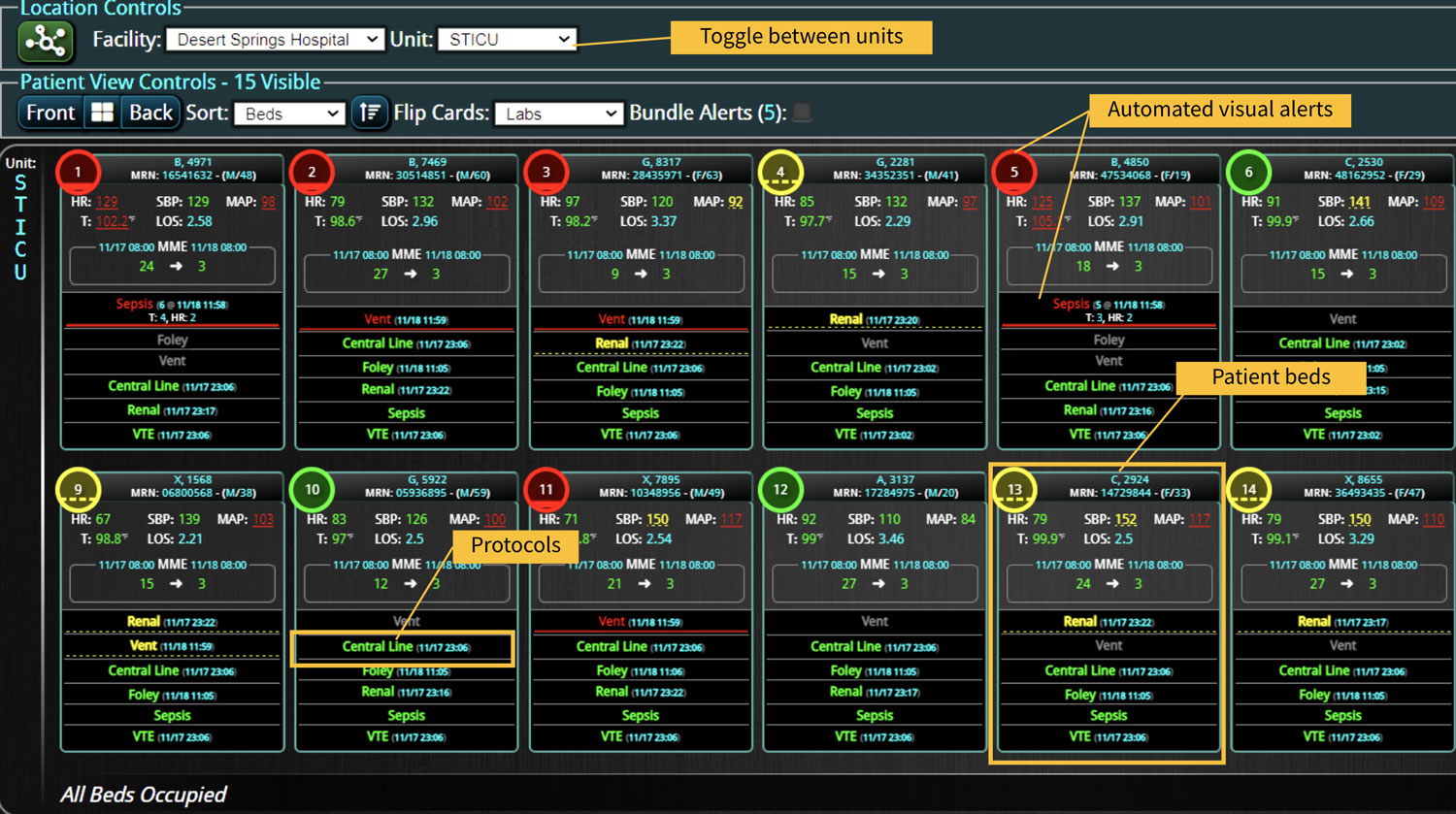
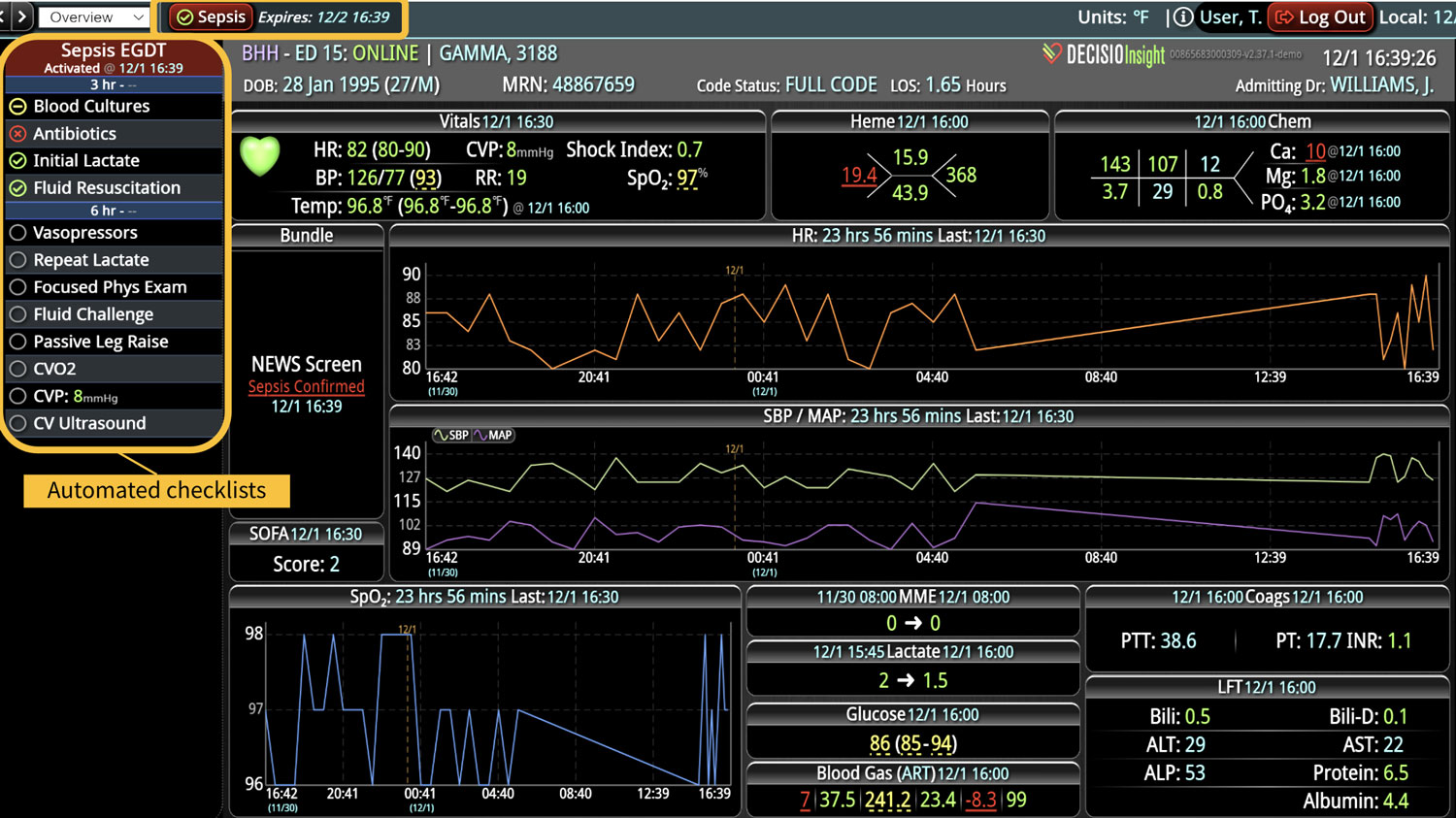
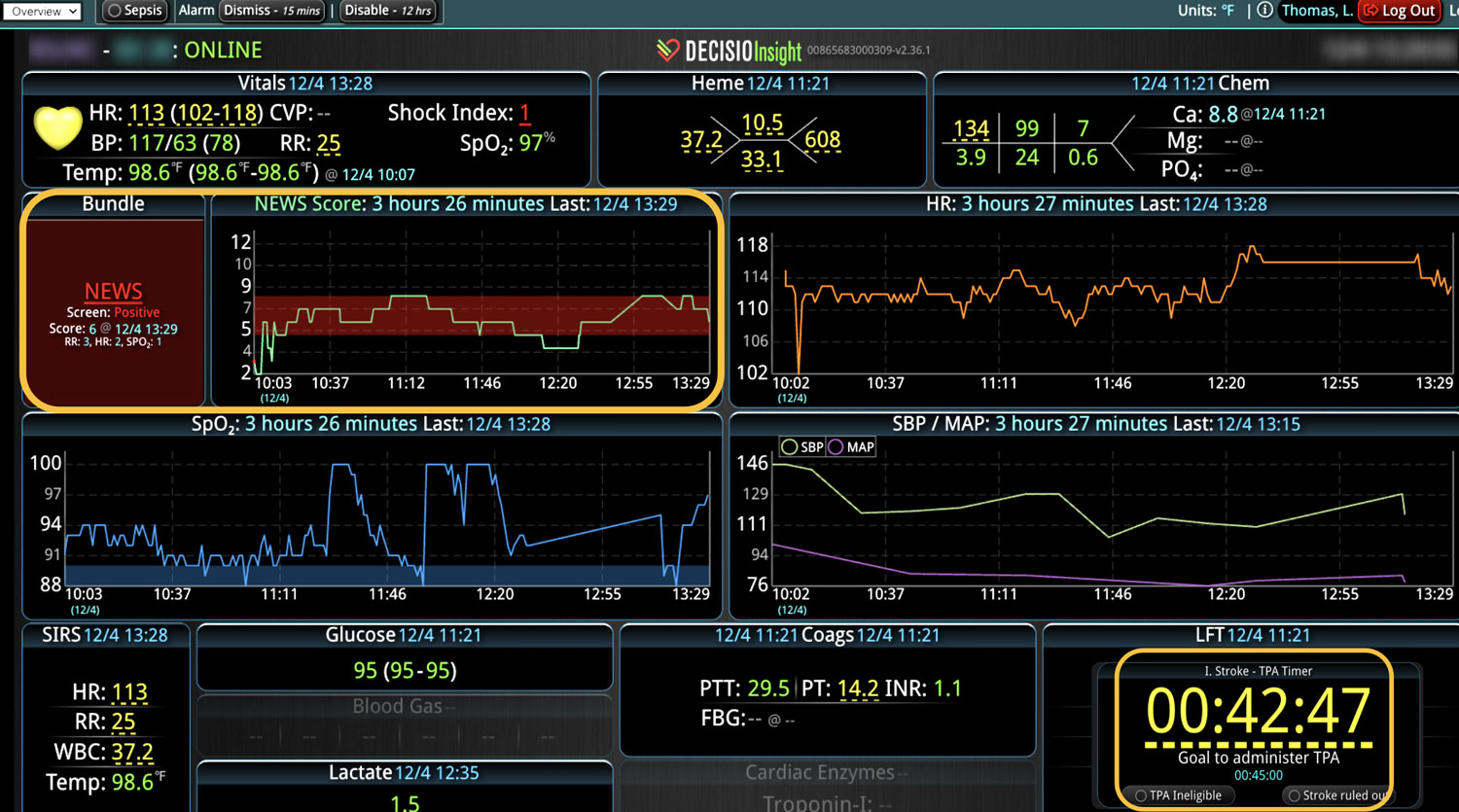
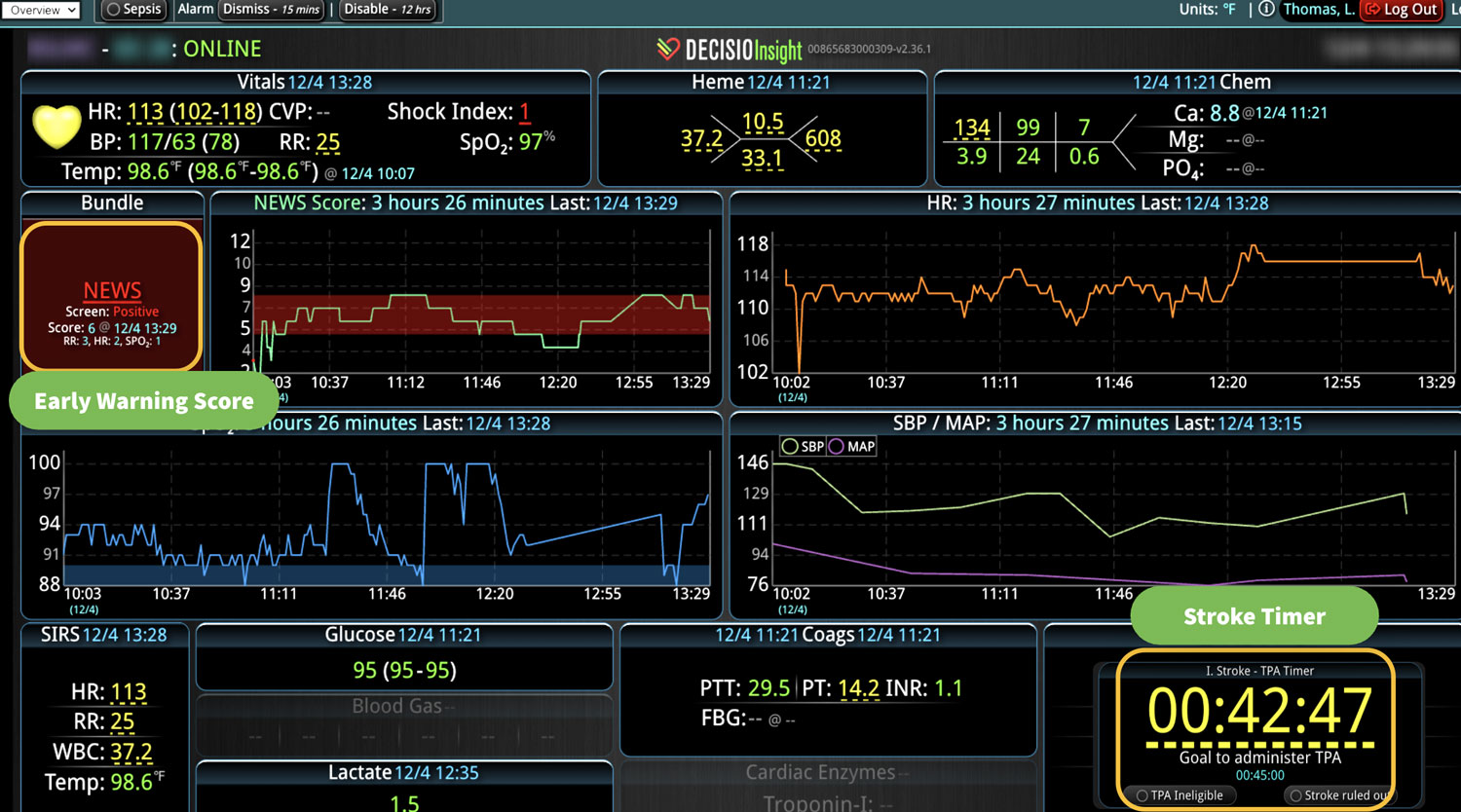
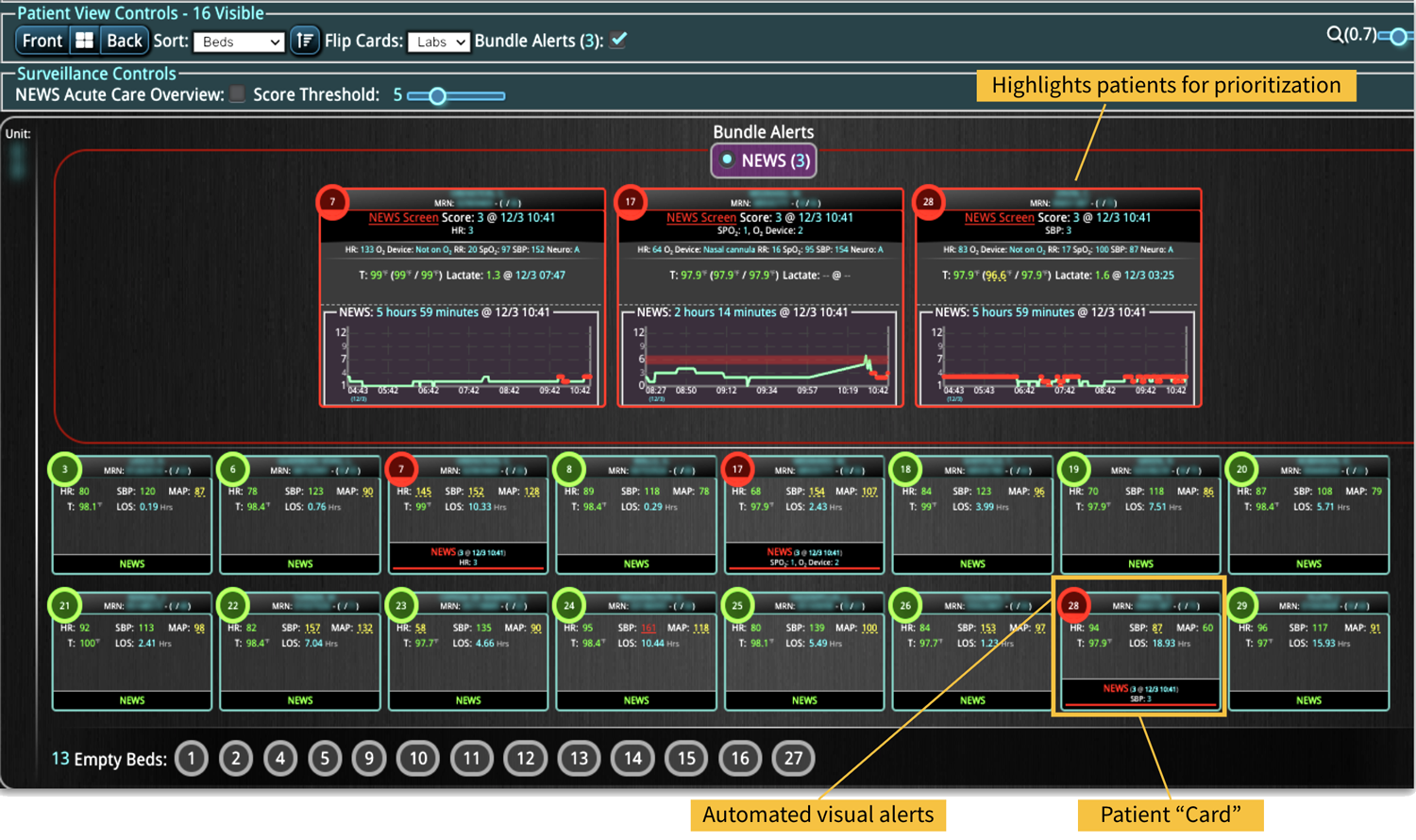
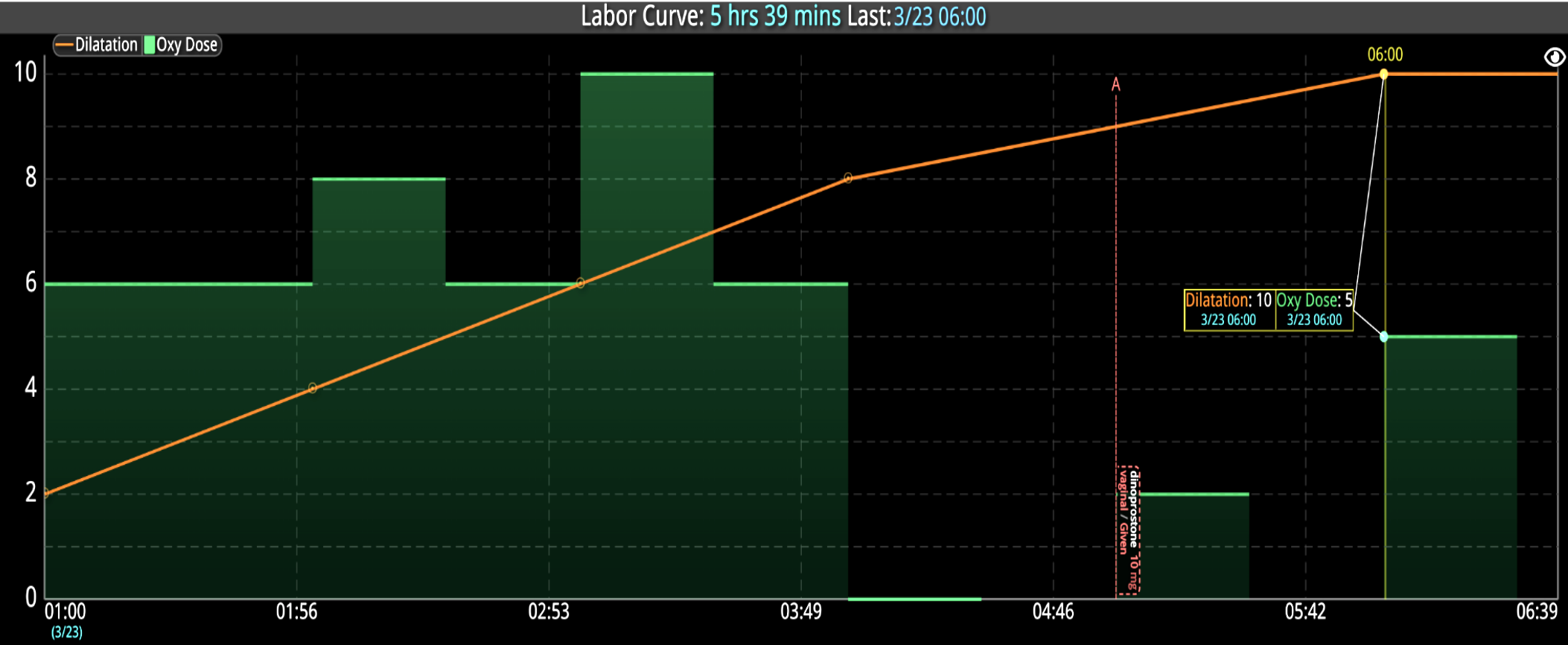
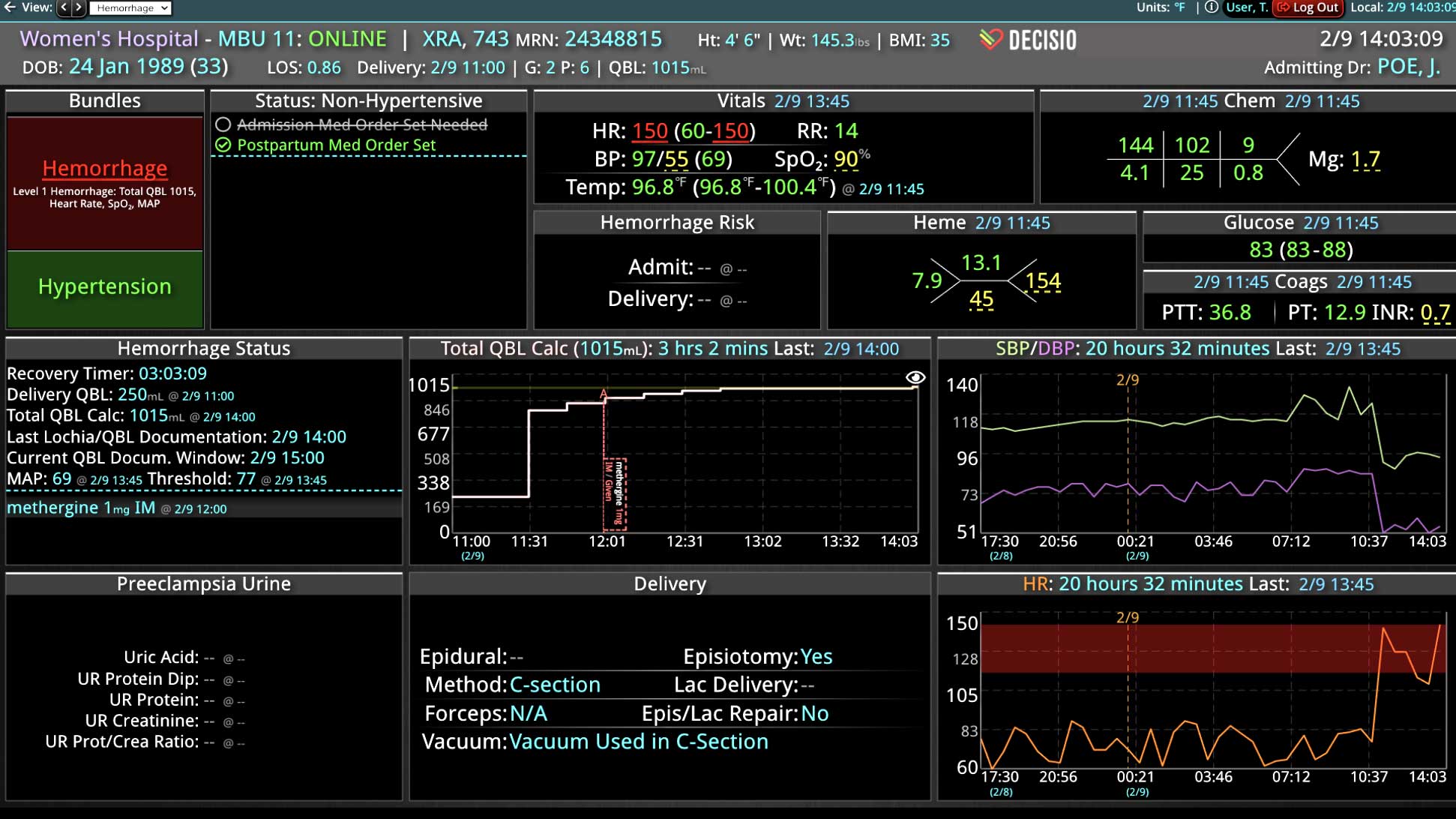
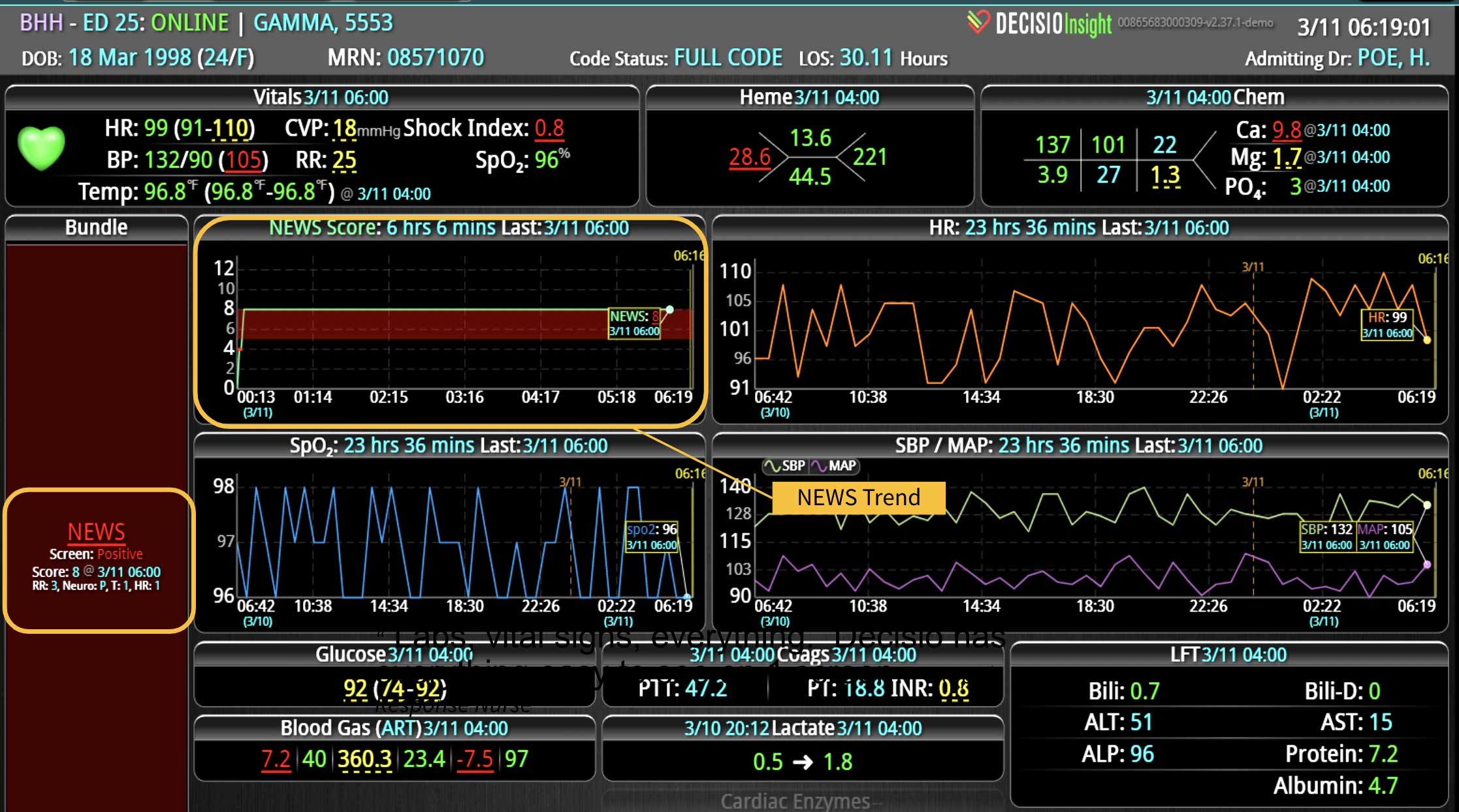
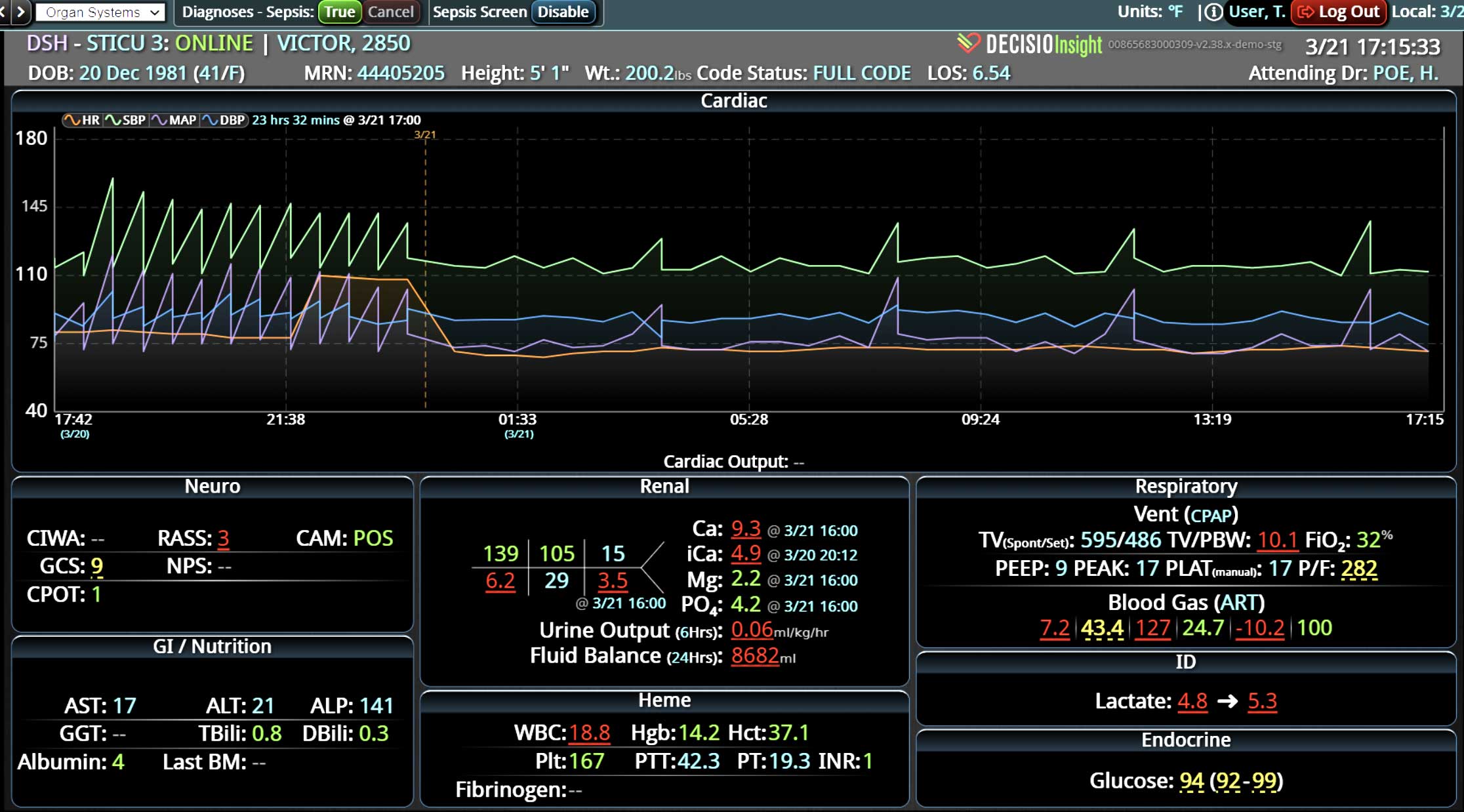
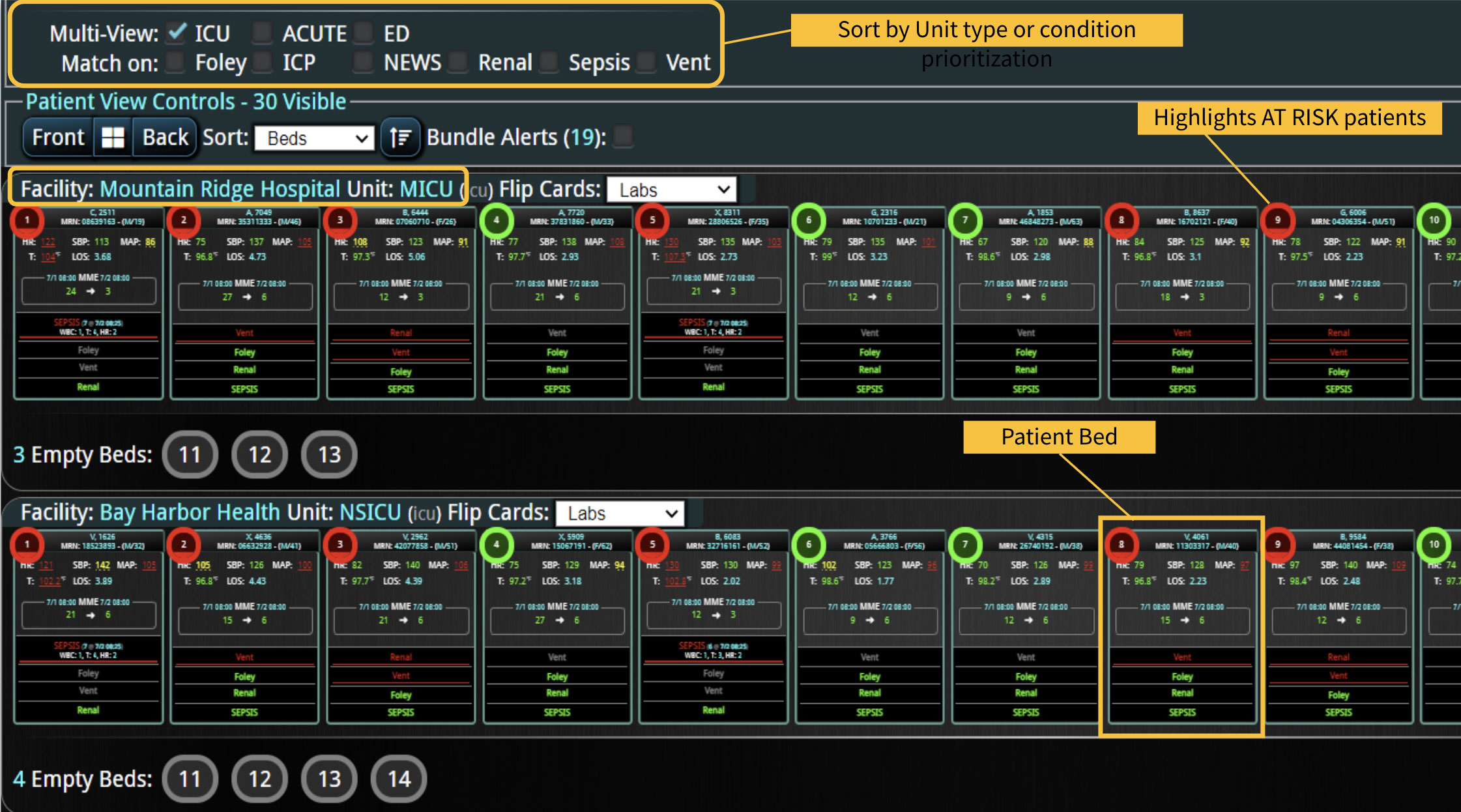
And yet, some hospitals are racing past “forward-thinking” on their way to “care transforming.” These hospitals have found an even better way: combining provider decision support tools and family-facing digital tools to establish the best of both worlds. For example, some institutions are implementing technology that provides a near real-time view of the patient’s story at the bedside and includes simplified displays of status changes. This dashboard is then shared by the care team, the patient, and the family. It enables the care team to make rapid treatment decisions and empowers family members to track their loved one’s progress – all while fostering a PFCC model rooted in trust.
Learn more About How we help clinicians improve patient outcomes
Schedule a call with our team to discuss how we are helping our clients revolutionize how clinicians manage patient interventions.